The Great Awakening-In God We Trust
FROM MERCOLA MEDICAL GASLIGHTING

STORY AT-A-GLANCE
- The medical industry has a vested interest in concealing injuries from its products
- A cruel but common method for accomplishing this is medical gaslighting
- Two of the most common diagnoses use to gaslight patients severely injured by the COVID-19 vaccines are "anxiety" and "functional neurologic disorder"
- Most doctors do not intend to gaslight their patients, but this behavior is an almost inevitable consequence of of their training and the modern practice of medicine. A patient understanding their perspective helps make it possible for doctors to see that patient's medical injuries
One of the classic ways an abuser controls their prey is to manipulate the environment so that the abused individual begins doubting their own observations regardless of what is occurring in front of them.
In the 1944 movie, Gaslight, this was accomplished by the villainous husband (played by Charles Boyer) adjusting the intake to gas-powered lights (causing them to flicker) and simultaneously denying that any change was occurring to his mentally abused wife (played by Ingrid Bergman). The term gaslighting originated from this classic movie.
In modern times, this is accomplished by having medical providers all echo the same message that a patient’s injury has nothing to do with the pharmaceutical (or other medical procedure in question). Most commonly, it instead is argued that the symptoms they are experiencing are due to pre-existing psychiatric issues the patient has (e.g., anxiety), which are treated with medications that often create additional issues.
Before we go any further, I want to emphasize just how miserable this is to go through as an injured patient. Imagine what it would be like if (due to the medical injury) the world you had previously known collapsed around you and every single person you trusted (including your friends and family who defer to the judgment of “experts”) told you that it was all in your head and you just needed psychiatric help. It’s a perfect recipe for going insane.
For example, let’s consider the recent experiences of Maddie De Garay in the pivotal Pfizer trial that was used to argue for the safety of the COVID-19 vaccines in the adolescent population:
Pfizer's trial only vaccinated 1,131 children so a single serious injury would have made the vaccine too dangerous.
— Pierre Kory, MD MPA (@PierreKory) January 11, 2023
Maddie's story shows just how far medicine will go to betray and gaslight patients who threaten its narrative. We may never know who else was swept under the rug. pic.twitter.com/4ONwty5Hu6
Note: This was clipped from episode 280 of the Highwire which we shortened (e.g., much of what she had to deal with in the hospital was cut out) so her story could reach a broader audience.
Although Maddie’s experience was atrocious, it was sadly not unique and many others had similar experiences in the COVID-19 vaccine trials. Similarly, I have heard many similar stories from other people who were harmed by the medical system.
Pharmaceuticals are inherently toxic. For example, most medications work by inhibiting enzymes (which are essential for life) and because of how interconnected the body is, this inhibition will create a variety of unintended consequences.
Similarly, most vaccinations function by making the immune system (often with the aid of toxins that help provoke that response) have an unnatural and narrowly focused response to a target substance.
The creation of this immune response unfortunately also often creates dysregulation within the immune system as this provocation can cause the immune system to be diverted away from attacking things it is supposed to address (e.g., microbes and cancers), while simultaneously triggering it to attack the body’s own tissue.
Since toxicity has always been inherent to the practice of allopathic (Western) medicine, the profession has gradually come up with a playbook to prevent its inevitable medical injuries from sabotaging business. This has essentially been accomplished by doing the following:
•Telling patients the adverse events they experienced either are not occurring or are unrelated to the toxic pharmaceutical.
•Developing an elaborate scientific apparatus that provides evidence refuting the link between these injuries and pharmaceuticals on the market, while concurrently training the population to defer to the scientific consensus rather than trusting their own observations.
•Making competing forms of medicine that lack a similar degree of inherent toxicity illegal, therefore making the only choice within the existing medical monopoly be a toxic form of medicine (similarly consider how allopathic medicine is always considered to be the best form of medicine every other approach must find a way to measure up to).
This is also why we have the doctrine in allopathic medicine that every treatment has risks and the treatments are chosen because its benefits outweigh its risk (as opposed to just exploring systems of medicine without those risks).
All of this in turn results in the tragic phenomenon known as medical gaslighting, or as some like to put it “allopathic medicine gaslights you to death.”
Why Can’t Doctors Diagnose Medical Injuries
I have found numerous documented examples of medical gaslighting stretching back to the late 1700s and in each case, typically only a minority of the medical profession is willing to acknowledge the injuries that are occurring could be linked to their pharmaceuticals.
At the same time, it’s rare for me to meet doctors I consider to be evil; on the contrary, most tend to be remarkably intelligent and well-intentioned individuals who genuinely want the best for their patients.
At this point, I believe medical gaslighting is a natural consequence of our training. Since the therapeutic toolbox of allopathic medicine is quite limited, most doctors cannot practice their craft without administering unsafe pharmaceuticals to their patients, and thus for the sake of their self-identity, they must fully believe in their pharmaceuticals (this subject was discussed further here).
It is an enormous personal investment to become a physician and it is extremely difficult for someone who goes through that to acknowledge that much of what they learned is highly questionable.
Similarly, no well-intentioned doctor wants to harm a patient, and since they often do, the reflexive psychological coping mechanism is to deny the possibility of each injury that occurs (discussed further here).
This first dawned on me at the start of my medical education when one of our professors inserted a tirade against anti-vaxxers into his lecture and concluded his argument with “… and just think about it. Do you really think pediatricians would vaccinate their patients if they thought vaccines could harm them?”
Although widespread denial of the harms that Allopathy causes likely explains some of my profession’s predilection for gaslighting, I do not believe it is the primary issue. Instead, I believe it is a result of the training doctors receive making them unable to recognize medical injuries.
The Origins of Medical Blindness
Because the human body is immensely complex, humans in every era face significant difficulties in being present to everything that is occurring within a human being. Most medical systems address this challenge by creating diagnostic models which simplify the immense complexity present in each patient down to the key things that must be focused upon to positively affect patient wellbeing.
The downside to this approach is that there will always be things in each patient that lie outside the diagnostic model being used to evaluate them. When this happens, those things understandably will not be recognized (unless the medical practitioner innately can perceive a complexity that transcends the limitations of their diagnostic model, something the majority of the population is not capable of).
In the case of allopathic medicine, we are taught a diagnostic model that is excellent for identifying many things (particularly indications for prescribing pharmaceutical drugs). However, our model also fails to notice many other things which are critical for health and wellness.
For example, much of medicine is taught by having a series of lists to memorize that are plugged into linear algorithms. Because this requires breaking many complex subjects into a binary “yes” or “no,” many important things that lie between these two polarities get lost in translation.
This is the easiest to illustrate with the nervous system (but the issue is by no means exclusive to it). When evaluating it, one of the things we are all taught to do is quickly check if the twelve cranial nerves are functioning normally (e.g., can you swallow, make a smile, or follow a finger with your eyes).
Frequently, although the cranial nerves are “generally normal” they will have some difficulty firing (e.g., at some point in the motion arc as the eyes travel side to side, they will jump instead of moving smoothly). These “minor” deficits often have a significant impact on a patient’s quality of life, but in most cases (except when evaluated by certain neurologists or neurosurgeons), the function of those nerves will be noted as normal and ignored.
One of the most common signs of a vaccine injury is a subtle cranial nerve dysfunction (discussed further here). While these are very easy to recognize if you are trained to look for them, that training does not exist within allopathic medicine, and as a result, most physicians simply cannot see the large number of vaccine injuries occurring around them.

Download this Article Before it Disappears
Download PDFSimplifying Illness
The cranial nerve example unfortunately is only one of many areas where a complex presentation of symptoms is simplified into a box that excludes an inconvenient diagnosis from ever being recognized. Another common way this boxing occurs is when an authoritative diagnosis is used to define a complex phenomenon without actually stating what it is.
For example, many disorders in medicine are simply symptoms written in Latin. Dermatitis quite literally translates to “inflammation of the skin,” and in most cases is simply treated with a cream that suppresses that inflammation.
Conversely, in many other medical systems, inflammation of the skin is recognized as an important sign of something being awry in the body, and the exact character and location of the inflammation are focused upon to identify and address the root cause of that inflammation (to some extent this is recognized in dermatology, but even there it occurs nowhere to the degree that it should).
Similarly, “migraine” headaches, although not exactly Latin, falls into a similar boat. While many things can cause migraines (e.g., they are very frequent after COVID-19 vaccine injuries) their cause is rarely focused upon, and instead, the standard medical approach is to throw pharmaceuticals at them until something improves the headache.
In my medical practice, I frequently treat migraines. In these patients, I find over and over that they have seen numerous doctors (including highly regarded specialists). Despite this, it is very rare anyone they saw was able to recognize the diagnostic signs or aspects of their history that point to the root actual cause of their headaches, and thus, not surprising that they will simply be prescribed more and more medications in the hope one will work.
Framing the Iatrogenic Debate
Iatrogenesis is the term for any type of illness or medical complication resulting from a bad reaction to medical care (e.g., a complication from a surgery or a pharmaceutical). A common pattern I’ve observed for decades is everyone denying a particular iatrogenic complication exists (e.g., “there is no evidence”), and then once overwhelming evidence exists that it does, it will be acknowledged.
Once this happens, the harm from the drug will be reframed so that only the accepted harm can be bad and an underlying assumption is created that nothing else is a possible complication.
For example, fluoroquinolones (e.g., Cipro) are fairly toxic antibiotics that can severely harm people and are frequently given for many minor infections (e.g., urinary tract infections) where their corresponding toxicity is simply not justified.
In medical school, everyone learns that a tendon rupture (something unique and hard to ignore) is a side effect of these drugs, and as a result, when doctors evaluate for harms, they will look for that but not be able to recognize most of the other well-documented complications from them.
My favorite recent example of this reframing occurred with the J&J COVID-19 vaccine. At the start of Operation Warp Speed, I hypothesized that a major goal was to get mRNA technology onto the market since it held the promise of trillions of dollars in future revenue for the pharmaceutical industry (but since there were safety challenges with it, nothing short of an "emergency" would be able to break the barrier to human testing).
Because of this, I suspected that once vaccine safety concerns emerged, a non-mRNA COVID-19 vaccine would be thrown under the bus to make the mRNA technology look “safe.” This is what then happened with the J&J vaccine when six cases of an extremely unusual blood clot being linked to that vaccine caused the FDA and CDC to pause its administration for 11 days.
By doing so, it created the perception the FDA was monitoring for vaccine side effects with a fine-tooth comb and was willing to pull the vaccine if it caused a rare side effect in a very small number of people.
Nothing could be further from the truth as the mRNA vaccines have caused far more blood clots than the J&J vaccine. Similarly, investigation after investigation shows the FDA is ignoring the endless deluge of red flags from the COVID-19 vaccines.
Unfortunately, this ploy worked, and in the odd instances where I hear a doctor willing to debate the safety of the vaccines, one of the most common arguments they still utilize is that if the FDA was willing to temporarily pause J&J after six blood clots, there is no possible way a larger unaddressed problem exists with the mRNA vaccines.
Psychiatric Complications and Iatrogenic Injuries
As the above points have shown, a variety of factors work against doctors being able to recognize the presence of medical injuries. The question then becomes, how will the injuries that inevitably occur be explained?
As you might imagine, the default strategy is to fold the injury into an amorphous diagnosis which (instead of allopathic medicine) can take the blame for the medical injury and then put that label on everyone with the injury. Typically this is done with psychiatric diagnoses, but recently COVID-19 infections have also been appointed to that role (both of these diagnoses were used to gaslight patients in the clinical trials for those vaccines).
The earliest references to this gaslighting I have found were at the time of Freud, where his new model of psychoanalysis was used to explain the complex symptoms observed within patients doctors otherwise had difficulty making sense of. However, as detailed in The Age of Autism: Mercury, Medicine, and a Man-Made Epidemic, an outside evaluation of Freud’s case studies suggests those patients’ problems actually arose from mercury poisoning.
Mercury, despite being extremely toxic, was used by the medical profession for centuries (and to some extent still is). Frequently, individuals with mercury poisoning would develop a wide array of complex diseases which included neurological and psychiatric complications (which like many other conditions were often attributed to “female hysteria”).
Freud’s message that these complications were the fault of the patient (e.g., as a result of unresolved sexual desires) rather than the physician was an immensely appealing message to the medical profession, and as a result, became the party line.
Ever since this time there has been a systemic failure to recognize that neurologic damage can produce psychiatric symptoms. Instead, neurologic symptoms are viewed as a manifestation of a pre-existing psychological illness that must be treated with psychological counseling and psychiatric medications.
One of the best examples of this issue is “Functional Neurological Disorder” (FND) which recognizes that something is wrong with the brain, but since no explanation can be found, it is assumed to have been due to pre-existing psychiatric conditions.
If you review the National Institute of Health’s description of FND, you will see that the above description is no exaggeration, and it is extremely sad to hear about the experiences vaccine-injured patients go through since FND is one of the most common diagnoses they receive.
When I look at FND cases, the cause of the disorder (e.g., seizures) can frequently be found, but since neurologists (including friends of mine) do not want to consider the actual cause, the tests needed to diagnose it are often not ordered or even known about by the doctors attending to the patient.
If you review Maddie’s story, you will note that this is also exactly what happened to her and her permanent paralysis from the vaccine was labeled as FND resulting from a psychiatric condition. Because of this gaslighting, she was not able to get appropriate care when her neurological reaction to the vaccine was occurring (that would have prevented permanent disability).
I believe this occurred because the chief investigator was fully aware that a severe neurologic reaction to a single participant would have made the vaccine too dangerous for children to take, so he decided to gaslight Maddie so her injury would not need to end up in the trial. Sadder still, Maddie’s experiences were not unique, and their experiences that indicate systemic fraud in the vaccine trials were detailed here.
Another common symptom doctors place the blame for medical injuries on is “anxiety.” The two major problems with this process are:
- Failing to recognize that having a life-changing injury will normally create distress, and similarly failing to recognize that being collectively gaslighted by medical providers is not good for anyone’s mental health.
- Pharmaceutical injuries frequently cause tissue damage that will trigger anxiety.
Sadly, very few doctors recognize that damage to the nervous system (which is a common toxicity of pharmaceuticals) can also create psychiatric disturbances. Instead, they only can recognize that psychiatric distress can often worsen neurologic symptoms, but do so without also realizing that it is much rarer for psychiatric distress to be the originating cause of a neurologic issue.
Similarly, many common psychiatric disorders have organic causes (e.g., chronic undiagnosed infections, traumatic brain injuries, or nutritional and metabolic deficiencies). However, in most cases, psychiatrists prescribe medications based on the symptoms a patient presents with (e.g., you are depressed so you need Prozac) rather than looking at the underlying cause.
I believe this is because doing the former pays well but the latter typically does not and is not emphasized in a psychiatrist’s training.
In addition to neurological damage frequently creating psychiatric complications (e.g., vagal dysfunction creating anxiety), damage to other organ systems can as well (Chinese medicine does an excellent job of mapping these correlations out). One of the best examples I have seen with the COVID-19 vaccines relates to the heart and I have had variations of the following conversations multiple times since 2021:
Friend: I have been having severe anxiety attacks since I got the vaccine. My heart starts beating rapidly, and I start to have pain in my chest. I never had this problem before, but now everything makes me anxious and it’s so hard for me to be calm.
Me: You should get your heart looked at.
Friend: What do you mean? Everyone told me it was anxiety due to stress.
Me: Trust me, you need to get your heart looked at.
(Time passes)
Friend: How did you know I had myocarditis?
Damage to the heart (or the vagus nerve) will often create an irregular heart rate and chest pain, and these palpitations often provoke anxiety. Unfortunately, since these symptoms are also triggered by anxiety, when they are observed, doctors will often default to a diagnosis of anxiety and look no further.
Conclusion
There are essentially two models of medical practice which are followed:
- The paternalistic model (where you are expected to unquestioningly trust and comply with everything the doctor tells you).
- The collaborative model where the physician is your partner in working towards health.
Although the paternalistic model was the standard for most of allopathic medicine’s history, in recent times, there has been a push for the collaborative model. Presently, many patients are seeking out collaborative physicians (especially since system doctors have to spend so much time going through checklists that there is little time for actual engagement with their patients), and the market is economically rewarding physicians who are making this change.
A key misconception much of the public holds about doctors is that we are infallible beings (which is a key justification for the paternalistic model). In reality, once you peer behind the lab coat, we struggle with many of the same issues you all do too. Being able to genuinely recognize this and respectfully treat the physician you see as a fellow human being is one of the most effective strategies for initiating a collaborative doctor-patient relationship.
Although doctors sometimes gaslight injured patients for self-serving reasons (e.g., to protect Pfizer’s vaccine in its clinical trials or under the misguided belief it will protect a doctor from a lawsuit), I believe the majority of cases occur because the doctors simply cannot see the injury occurred. As a result, these doctors believe they are doing the best for the patient when in reality they are just gaslighting them.
One of the largest issues in our modern era is how disconnected we have become from ourselves and others. Within the doctor-patient relationship, this disconnection makes it much less likely a physician will be able to recognize what is happening in a patient (e.g., a medical injury) or feel compelled to go to bat for them while every other healthcare provider is gaslighting them.
When people ask me for their best options to avoid being gaslighted, I thus suggest pursuing one of the following options:
1)See a physician who you pay directly (rather than one who takes insurance). This business model matters because it forces the doctor to have a collaborative doctor-patient relationship and stay in business (no one will pay to see them if they just get gaslit). I am a big believer in the statement “you get what you pay for” and if only see system doctors who base their practice around insurance payments, you often do not get a good outcome.
For example, I had a patient recently who I felt exemplified this issue. He had what I felt was a relatively straightforward problem that had significantly impacted his life for 25 years. When I reviewed his history, he told me he had seen a dozen (insurance-taking) doctors, many of whom promised they could fix the problems with elaborate procedures from their specialty (all of which did nothing or made his issue worse).
What was striking about his story was that only one of them had ever even performed an extensive evaluation (e.g., talking with him about the history of his disease) to try to figure out what was causing the problem.
2)However, while seeing a private-pay physician often is an excellent investment, many patients simply cannot afford to do so. In this case, the ideal scenario is to find an insurance-taking physician through word of mouth who has earned a reputation for forging collaborative doctor-patient relationships. Unfortunately, these recommendations are hard to come across and typically these doctors will have full practices that are hard to get into.
3)The third (and often the only available option is to take the initiative to forge a collaborative relationship with the doctor through having a respectful demeanor where you treat the doctor as a fellow human being rather than “the doctor.”
In general, this approach will be the most effective on doctors who recently completed their medical training (everyone becomes more rigid with age, plus their practices are not yet full), and in medical settings where the doctors get longer per visit (you can’t really build a collaborative relationship in 10-15 minutes).
Regardless of the option you choose, it is also often important to provide the documentation to support the occurrence of your medical injury. This includes records establishing a timeline of the injury following the medical therapy and scientific literature substantiating the link between the two.
Physicians in turn (especially younger ones) will be the most receptive to considering this link if it is presented in a composed and thoughtful way rather than a confrontational manner, because like every other human they tend to become defensive. Given how upsetting the process of being gaslighted is, maintaining this demeanor can be extremely challenging.
Sadly though, it is necessary because doctors are trained to see these injuries as being psychological in nature, and a patient expressing their completely justifiable feelings about the situation will often feed into the doctor’s erroneous perceptions about the patient’s mental health.
About the Author
A Midwestern Doctor (AMD) is a board-certified physician from the Midwest and a longtime reader of Mercola.com. To find more of AMD's work, be sure to check out The Forgotten Side of Medicine on Substack.
Views: 37
Comments are closed for this blog post
-
Comment by carol ann parisi on February 8, 2023 at 4:57pm
-

-
-

-
-
-
-
The Fauci Files
- Dr. Anthony Fauci has served as the director of the National Institute of Allergy and Infectious Diseases (NIAID) since 1984, but has yet to come out with the “Big One” — a vaccine or infectious disease treatment that will allow him to retire with a victory under his belt
- Fauci has flip-flopped on the use of masks, first mocking people for wearing them, and then insisting they should. In mid-July, he suddenly urged governments to “be as forceful as possible” on mask rules
- While Fauci still claims there’s only anecdotal evidence supporting the use of hydroxychloroquine, and that the drug doesn’t work for COVID-19, the scientific support for it goes as far back as 2005
- In April, Fauci praised the NIAID-sponsored drug Remdesivir, saying it "has a clear-cut and significant positive effect in diminishing the time to recovery." Overall, the improvement rate for the drug was 31%
- Research now shows hydroxychloroquine reduced mortality by 50% when given early, and many doctors anecdotally claim survival rates close to 100%. Despite such excellent results, Fauci continues to disparage and cast doubt on hydroxychloroquine
From Dr. Joseph Mercola
Since COVID-19 first entered the scene, exchange of ideas has basically been outlawed. By sharing my views and those from various experts throughout the pandemic on COVID treatments and the experimental COVID jabs, I became a main target of the White House, the political establishment and the global cabal.
Propaganda and pervasive censorship have been deployed to seize control over every part of your life, including your health, finances and food supply. The major media are key players and have been instrumental in creating and fueling fear.
I am republishing this article in its original form so that you can see how the progression unfolded.
Originally published: September 1, 2020
At 79 years old, Dr. Anthony Fauci — who has served as the director of the National Institute of Allergy and Infectious Diseases (NIAID) since 1984 — has yet to come out with the “Big One” — a vaccine or infectious disease treatment that will allow him to retire with a victory under his belt.
He failed to create a successful vaccine for AIDS, SARS, MERS and Ebola. A COVID-19 vaccine is essentially his last chance to go out in a blaze of glory. As evidenced by his history, he will stop at nothing to protect Moderna’s COVID-19 vaccine and Gilead’s antiviral Remdesivir.
He even threw tried and true pandemic protocols out the window when COVID-19 hit, turning into an unquestioning spokesman for draconian liberty-stripping measures instead. To echo a question asked by Dr. Sal Martingano in his article,1 “Dr. Fauci: ‘Expert’ or Co-Conspirator,” why are we not questioning this so-called expert?
Fauci ‘Has Been Wrong About Everything’
The risk we take when listening to Fauci is that, so far, he’s been wrong about most things. In a July 14, 2020, “Opposing View” editorial in USA Today, White House adviser Peter Navarro, director of the Office of Trade and Manufacturing Policy, stated that Fauci “has been wrong about everything that I have interacted with him on.”2 According to Navarro, Fauci’s errors in judgment include:3
•Opposing the ban on incoming flights from China in late January 2020.
•Telling the American people the novel virus outbreak was nothing to worry about well into February.
•Flip-flopping on the use of masks — first mocking people for wearing them, and then insisting they should. In fact, mid-July, he suddenly urged governments to “be as forceful as possible” on mask rules.4
•Claiming there was only anecdotal evidence supporting the use of hydroxychloroquine, when the scientific grounds for it go as far back as 2005, when the study,5 “Chloroquine Is a Potent Inhibitor of SARS Coronavirus Infection and Spread,” was published in the Virology Journal.
Fauci should have been well aware of this publication. According to that study,6 “Chloroquine has strong antiviral effects on SARS-CoV infection of primate cells. These inhibitory effects are observed when the cells are treated with the drug either before or after exposure to the virus, suggesting both prophylactic and therapeutic advantage,” the study authors said. In other words, the drug worked both for prevention and treatment.
As noted by Navarro, more recent research found hydroxychloroquine reduced the mortality rate among COVID-19 patients by 50% when used early.
Interestingly, in a March 24, 2020, interview7 with Chris Stigall, Fauci did say that — were he to speak strictly as a doctor treating patients — he would certainly prescribe chloroquine to COVID-19 patients, particularly if there were no other options.
Then, in August, he flipped back to insisting hydroxychloroquine doesn’t work,8 even though by that time, there were several studies demonstrating its effectiveness against COVID-19 specifically.
So, it appears Fauci has had a hard time making up his mind on this issue as well, on the one hand dismissing the drug as either untested or ineffective against COVID-19, and on the other admitting it would be wise to use, seeing how the options are so limited.
Navarro continues:9
“Now Fauci says a falling mortality rate doesn’t matter when it is the single most important statistic to help guide the pace of our economic reopening. The lower the mortality rate, the faster and more we can open. So when you ask me whether I listen to Dr. Fauci’s advice, my answer is: only with skepticism and caution.”
Fauci Has Done Nothing to Help Unite the Country
While Fauci claims to be exasperated by how political the pandemic has become,10 before Instagram banned him from the platform and took the post down,11 Robert F. Kennedy Jr. pointed out in an August 2, 2020, Instagram post12 that Fauci himself is, at least in part, part of the problem, as his double standards on hydroxychloroquine have done much to polarize and divide the nation:
“Fauci insists he will not approve HCQ for COVID until its efficacy is proven in ‘randomized, double blind placebo studies.’ To date, Dr. Fauci has never advocated such studies for any of the 72 vaccine doses added to the mandatory childhood schedule since he took over NIAID in 1984. Nor is he requiring them for the COVID vaccines currently racing for approval.
Why should chloroquine be the only remedy required to cross this high hurdle? HCQ is less in need of randomized placebo studies than any of these vaccines since its safety is well established after 60 years of use and decades on WHO’s listed of ‘essential medicines.’
Fauci’s peculiar hostility towards HCQ is consistent with his half century bias favoring vaccines and patent medicines. Dr. Fauci’s double standards create confusion, mistrust and polarization.”
In a June 10, 2020, article,13 Global Research also questioned Fauci’s many attempts to disparage the drug for no apparently valid reason; even promoting the fake (and ultimately retracted) Lancet study that claimed to show hydroxychloroquine was dangerous. At the end of the day, who benefits? Well, certainly it benefits the drug and vaccine industries, which seems to be where Fauci’s loyalties lie.
Download this Article Before it Disappears
Download PDFFauci’s Bias Is Hard to Miss
While Fauci is not named on the patents of either Moderna’s vaccine or Remdesivir, the NIH does have a 50% stake in Moderna’s vaccine,14 and the recognition that would come with a successful vaccine launch would certainly include Fauci.
He also has lots to lose — if nothing else, his pride — if Remdesivir doesn’t become a blockbuster, as his NIAID is sponsoring the clinical trials.15 The NIAID also supported the original research into Remdesivir, when it was aimed at treating Ebola.16
His bias here is clear for anyone to see. April 29, 2020, he stated17 Remdesivir "has a clear-cut and significant positive effect in diminishing the time to recovery." How good is that? Patients on the drug recovered in 11 days, on average, compared to 15 days among those receiving a placebo. Overall, the improvement rate for the drug was 31%.
Meanwhile, research18 now shows hydroxychloroquine reduced mortality by 50% when given early, and many doctors anecdotally claim survival rates close to 100%. This still isn’t good enough for Fauci, who continues insisting hydroxychloroquine is a bust.19
His stance on these two drugs certainly doesn’t make sense based on the data alone. But it does make sense if he wants (or has been instructed) to protect the profits of Remdesivir.
As director of NIAID, which has been part of Remdesivir’s development from the start, why wouldn’t he want to see it become a moneymaker for the agency he dedicated his career to? It also makes sense when you consider his primary job is to raise funds for biodefense research, primarily vaccines but also diagnostics and drug therapies.20,21
Fauci Doubts Safety of Russian Vaccine
Early in August 2020, Russia announced they would begin vaccinating citizens with its own COVID-19 vaccine, despite not finishing large-scale human trials.22 The announcement drew skepticism from American infectious disease specialists, including Fauci, who said he has “serious doubts” that Russia’s COVID-19 vaccine is actually safe and effective.23
Fauci conveniently ignores the many failed attempts to create other coronavirus vaccines over the past two decades, including vaccines against SARS and MERS.
He’s probably right on that point. It’s hard to imagine you can prove safety and effectiveness in a mere two months of trials. But the fast-tracked vaccine efforts of the U.S. and EU are hardly bound to be significantly better, considering the many shortcuts that are being taken.
Fauci Ignores Two Decades of Failed Coronavirus Vaccines
Despite being in a position to know better, Fauci conveniently ignores the many failed attempts to create other coronavirus vaccines over the past two decades, including vaccines against SARS and MERS. A paper24 by Eriko Padron-Regalado, “Vaccines for SARS-CoV-2: Lessons From Other Coronavirus Strains” reviews some of these past experiences. As noted in the Conservative Review:25
“Since their emergence in 2003 and 2012 respectively, no safe and efficacious human vaccines for either SARS-Cov1 or MERS have been developed.
Moreover, experimental non-human (animal model) evaluations of four SARS-Cov1 candidate vaccine types, revealed that despite conferring some protection against infection with SARS-Cov1, each also caused serious lung injury, caused by an overreaction of the immune system, upon viral challenge.26
Identical ‘hypersensitive-type’ lung injury occurred27 when mice were administered a candidate MERS-Cov vaccine, then challenged with infectious virus, negating the ostensible benefit achieved by their development of promising ... ‘antibodies’ ... which might have provided immunity to MERS-Cov.
These disappointing experimental observations must serve as a cautionary tale for SARS-Cov2 vaccination programs to control epidemic COVID-19 disease.”
NIAID Safety Controversies and Ethics Violations
When recently asked for a rebuttal to criticism of his leadership during the pandemic, Fauci replied, “I think you can trust me,” citing his long record of service in government medicine. However, that long service record is fraught with ethics and safety lapses.
For example, in 2005, NPR reported28 the NIH tested novel AIDS drugs on hundreds of HIV-positive children in state foster care during the late 1980s and90s without assigning patient advocates to monitor the children’s health, as is required by law in most states.
Fauci was appointed director of the NIAID in 1984. The AIDS research was part of his research portfolio, and the AIDS research division reported directly to him, so these violations occurred on his watch.29 In 2008, two NIH biomedical ethicists published a paper on the controversial practice of using wards of the state as guinea pigs, noting:30
"Enrolling wards of the state in research raises two major concerns: the possibility that an unfair share of the burdens of research might fall on wards, and the need to ensure interests of individual wards are accounted for ... Having special protections only for some categories is misguided. Furthermore, some of the existing protections ought to be strengthened."
Under Fauci, the NIAID became the largest funder of HIV/AIDS in the world.31 Despite that, numerous articles over the years have discussed how AIDS activists have been less than satisfied with Fauci and the NIAID.32,33,34 A 1986 article stated:35
“If Fauci were less intent on amassing power within the federal health bureaucracy ... he would have left AIDS treatment research with the NCI, where it began, relying on that institute's proven expertise in organizing large, multisite clinical trials for cancer therapies."
A July 23, 2020, article in Just the News lists several other safety and ethics problems that Fauci has been involved in through the years, including conflict of interest violations in vaccine research.36
Just the News also interviewed NIAID chief of ethics and regulatory compliance Dr. Jonathan Fishbein, whom the NIAID was forced to reinstate in 2005 after it was determined that Fishbein had been wrongly fired in retaliation for raising concerns about lack of safety in some of the agency’s research:37
“Fishbein said ... Fauci failed to take responsibility for the managers and researchers working below him when signs of trouble emerged, allowing problems to persist until others intervened. ‘Fauci is all about Fauci,’ Fishbein said. ‘He loves being the headline. It’s his ego.’”
Fauci’s Connections to Wuhan Lab
By now, you probably also know that the NIAID funded gain-of-function research on coronaviruses at the Wuhan Institute of Virology. As reported by Newsweek:38
“In 2019, with the backing of NIAID, the National Institutes of Health committed $3.7 million over six years for research that included some gain-of-function work. The program followed another $3.7 million, 5-year project for collecting and studying bat coronaviruses, which ended in 2019, bringing the total to $7.4 million.”
This money was not given directly, but rather funneled to the Wuhan lab via the EcoHealth Alliance. According to a recent report by The Wall Street Journal,39 the NIH is now insisting EcoHealth Alliance submit all information and materials from the Wuhan lab before it’s allowed to resume funding.
Fauci is a longtime proponent of dangerous gain-of-function research. In 2003, he wrote an article40 published in the journal Nature on how “the world needs new and creative ways to counter bioterrorism.”
“We will pursue innovative approaches for modulating innate immunity to induce and enhance protection against many biological pathogens, as well as simple and rapid molecularly based diagnostics to detect, characterize and quantify infectious threats,” Fauci wrote.
“These are lofty goals that may take many years to accomplish — but we must aspire to them. Third, we must enormously strengthen our interactions with the private sector, including biotechnology companies and large pharmaceutical corporations.
Many biodefence-related products that we are pursuing do not provide sufficient incentives for industry — the potential profit margin for companies is tenuous, and there is no guarantee that products would be used.
Therefore, we will seek non-traditional collaborations with industry, for example guaranteeing that products will be purchased if companies sign up ... so that we can quickly make available effective vaccines and treatments ...”
With that, there can be little question about which team Fauci is on. He’s on the side of drug and vaccine makers, and has been for decades. There’s no money to be made by either the agency or its private collaborators from natural products such as vitamin D, vitamin C, quercetin or its drug equivalent, hydroxychloroquine. All of these are dirt-cheap and off patent.
Prediction Track Record = Null
Fauci’s predictions for COVID-19 mortality have also turned out to be as inaccurate as all of his previous predictions. In 1987, he predicted heterosexual infection of HIV/AIDS would rise to 10% by 1991. It never rose above 4%.
He predicted the bird flu would result in 2 million to 7 million deaths. In the end, the avian H5N1 flu killed 440 worldwide. He sought billions of dollars to combat the threat of Zika, a virus that fizzled without making much of an impact anywhere.41
When you look at his track record, you realize he’s predicted “nightmare” scenarios for decades, none of which have materialized. Last but not least, Dr. Fauci serves on Bill Gates leadership council.
-
-

-
-

-
-
More Than 217,000 Americans Killed by the COVID Jab
Analysis by Dr. Joseph MercolaFact Checked
- February 07, 2023

STORY AT-A-GLANCE
- According to a December 2021 survey of 2,840 Americans, between 217,330 and 332,608 people died from the COVID jabs in 2021
- Survey results also show that people who got the jab were more likely to know someone who experienced a health problem from COVID-19 infection, whereas those who knew someone who experienced a health problem after getting the jab were less likely to be jabbed
- Of the respondents, 34% knew one or more people who had experienced a significant health problem due to the COVID-19 illness, and 22% knew one or more people who had been injured by the shot
- 51% of the survey respondents had been jabbed. Of those, 13% reported experiencing a “serious” health problem post-jab. Compare that to Pfizer’s six-month safety analysis, which claimed only 1.2% of trial participants experienced a serious adverse event
- In December 2022, Rasmussen Reports polled 1,000 Americans. In this poll, 34% reported experiencing minor side effects from the jab and 7% reported major side effects
While it's clear that the experimental COVID shots have killed a considerable number of people, the total death toll remains elusive, thanks to U.S. health agencies obfuscating, hiding and manipulating data.
That said, the most recent survey1,2 — published in the peer-reviewed journal BMC Infectious Diseases — puts the death toll from the COVID jabs somewhere between 217,330 and 332,608 in 2021 alone. As noted by Steve Kirsch:3
"[We've] killed at least 217,000 Americans and seriously injured 33 million … in just the first year, and the CDC and FDA want to give you more shots … Since deaths from the vaccine were higher in 2022, most experts would estimate the all-cause mortality death toll from the COVID vaccines to be in the range of 500K to 600K.
So the global cost of life from these vaccines is on the order of 10 to 12 million people … These [data] are consistent with the numbers I've been saying for a long time. It's not a coincidence."
Survey: Why People Did or Did Not Get the Jab
Now, the slant of this paper is kind of interesting. The primary aim of it was to "identify the factors associated by American citizens with the decision to be vaccinated against COVID-19."
The author was curious about why 31% of the U.S. population had declined the jab or not completed the primary series by November 2022, nearly two years into a massively advertised "vaccination" campaign.
Calculating the proportion of fatal events from the jab was secondary. As explained by the author, Mark Skidmore,4 Ph.D., an economics professor at Michigan State University:5
"A largely unexplored factor is the degree to which serious health problems arising from the COVID-19 illness or the COVID-19 vaccines among family and friends influences the decision to be vaccinated.
Serious illness due to COVID-19 would make vaccination more likely; the perceived benefits of avoiding COVID-19 through inoculation would be higher.
On the other hand, observing major health issues following COVID-19 inoculation within one's social network would heighten the perceived risks of vaccination. Previous studies have not evaluated the degree to which experiences with the disease and vaccine injury influence vaccine status.
The main aim of this online survey of COVID-19 health experiences is to investigate the degree to which the COVID-19 disease and COVID-19 vaccine adverse events among friends and family, whether perceived or real, influenced inoculation decisions. The second aim of this work is to estimate the total number of COVID-19 vaccine induced fatalities nationwide from the survey."
Here's an excerpt describing the methodology:6
"An online survey of COVID-19 health experiences was conducted. Information was collected regarding reasons for and against COVID-19 inoculations, experiences with COVID-19 illness and COVID-19 inoculations by survey respondents and their social circles. Logit regression analyses were carried out to identify factors influencing the likelihood of being vaccinated."
Survey Findings
A total of 2,840 people completed the survey between December 18 and 23, 2021. The mean age was 47, and the gender ratio was 51% women, 49% men. Just over half, 51%, had received one or more COVID jabs.
As Skidmore suspected, results showed that people who got the jab were more likely to know someone who experienced a health problem from COVID-19 infection, whereas those who knew someone who experienced a health problem after getting the jab were less likely to be jabbed.
Of the respondents, 34% knew one or more people who had experienced a significant health problem due to the COVID-19 illness, and 22% knew one or more people who had been injured by the shot. So, as noted by to the author:7
"Knowing someone who reported serious health issues either from COVID-19 or from COVID-19 vaccination are important factors for the decision to get vaccinated."
As for the types of side effects experienced by people within the respondents' social circles, they included (but were not limited to) the "usual suspects," such as:
- Heart and cardiovascular problems
- Severe COVID infection or other respiratory illness
- Feeling generally unwell, weak, fatigued and out of breath for weeks
- Blood clots and stroke
- Death
Download this Article Before it Disappears
Download PDFHundreds of Thousands Killed for No Reason
Based on these survey data, Skidmore estimates:
"… the total number of fatalities due to COVID-19 inoculation may be as high as 278,000 (95% CI 217,330-332,608) when fatalities that may have occurred regardless of inoculation are removed."
Were COVID-19 an infection with an extremely high mortality rate, perhaps high rates of death from a vaccine would be acceptable. But COVID-19 has an exceptionally low mortality rate, on par with or lower than influenza, hence the risk associated with the COVID jabs ought to be equally low.
The global cost of life from these vaccines is on the order of 10 to 12 million people. ~ Steve Kirsch
As it stands, the risks of the shots are very high, while Pfizer's own trial data, with more than 40,000 participants, show they offer no benefit in terms of your risk of hospitalization and/or death. The absolute risk reduction is so minute as to be inconsequential.8
High Rates of Side Effects
The death toll from the jabs isn't the only disturbing part of this paper, though. Skidmore's findings also suggest side effects from the jab may be more common than previously suspected.
As mentioned, 51% of the respondents had been jabbed. Of those, 15% reported experiencing a new health problem post-jab and 13% deemed it "serious." Compare that to Pfizer's six-month safety analysis,9 which claimed only 1.2% of trial participants reported a serious adverse event.
Now, as suggested by Kirsch,10 "we need to discount that by a factor of two because people report less severe adverse events as adverse events." Still, that means serious adverse events from the jab are five times higher than what Pfizer reported.
"This is why the FDA never does after-market surveys in the drugs it approves. Because reality hurts," Kirsch writes.11 "It is the FDA that should have discovered this before Mark Skidmore. The FDA is asleep at the wheel and they just believe everything the drug companies tell them, hook, line, and sinker. This is a major miss. Why aren't they doing surveys like this to see if the reality matches the study?"
More Side Effect Rate Comparisons
For additional comparison, here are the findings of several other investigations:
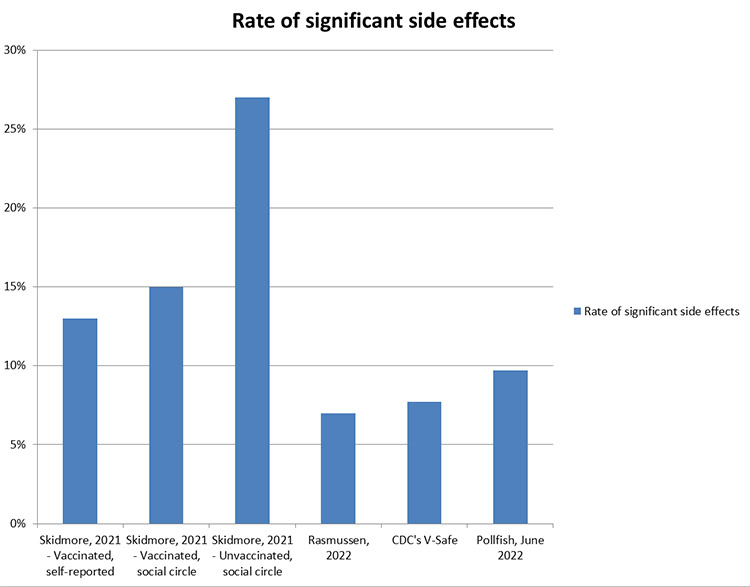
- Rasmussen Reports12 — In December 2022, Rasmussen Reports polled 1,000 Americans. In this poll — taken one year after Skidmore's survey — 34% reported experiencing minor side effects from the jab and 7% reported major side effects.
- CDC's V-Safe data13 — In October 2022, ICAN obtained the Center for Disease Control and Prevention's V-Safe data. This is a voluntary program to monitor adverse vaccine reactions. Of the 10.1 million COVID jab recipients who used the app, 7.7% had to seek medical care post-jab.
- Kirsch-funded survey14 — A June 2022 U.S. survey by the market research company Pollfish found that 16.3% of COVID jabbed respondents experienced an injury, and 9.7% required medical care.
The graphic below, which visually compares Skidmore's findings to the findings of the Rasmussen, V-Safe and Pollfish surveys, was created by InfoGame on Substack.15 As noted by InfoGame:
"Skidmore's article serves as another sign that the rate of COVID-19 side effects is extremely high and that the COVID-19 vaccines are an unprecedently risky medical product."
Menstrual Irregularities Are Common Post-Jab
While we're on the topic of reported side effects, several surveys have also focused on the frequency of abnormal menses in women who got the jab, which could be indicative of reproductive harm. For example:
- A British survey published in early December 2021 found 20% of women experienced menstrual disturbances following their jab.16
- A study published in Science Advances in mid-July 2022 found 66% of "fully vaccinated" postmenopausal women experienced abnormal breakthrough bleeding. In total, 42.1% reported heavier menstrual flow post-jab (this included women of all ages, as well as transgenders on hormone treatments).17
- An Italian peer-reviewed study published in March 2022 found that "50-60% of reproductive-age women who received the first dose of the COVID-19 vaccine reported menstrual cycle irregularities, regardless of the type of administered vaccine." After the second dose, abnormal menses were reported by 60% to 70%.18
People in High Places Seek Retraction
Not surprisingly, people in high places are already trying to force a retraction of the paper. A special notice from the editor, dated just two days post-publication, states, "Readers are alerted that the conclusions of this paper are subject to criticisms that are being considered by editors. Specifically, that the claims are unsubstantiated and that there are questions about the quality of the peer review." As noted by Kirsch:19
"They are actively trying to get the paper retracted because it destroys the narrative. I'm certain they will succeed because journals are under intense pressure to censor any anti-narrative paper. The problem is that Mark's survey was entirely consistent with my surveys.
If they want to have the paper retracted they need to show us THEIR surveys. But of course, they don't have any surveys because they are too afraid of the results.
So they will use hand-waving arguments like "I don't like the methodology" or some nonsense like that instead of gathering their own data. They will NEVER show us survey data that supports their narrative because it isn't there.
That's why there are no success anecdotes. NOBODY can give me the name of a US geriatric practice where all-cause deaths plummeted after the vaccines rolled out. In every case, they went the wrong way. The narrative is unraveling at an accelerated pace but the medical community is still fighting the truth."
-
-
USA Today Smears Mercola Over Vitamin C and D Information
Analysis by Dr. Joseph MercolaFact Checked
- February 06, 2023

STORY AT-A-GLANCE
- Mainstream media, supported by monopoly tech platforms like Google, YouTube, Facebook and Twitter, are going to great lengths to control the narrative of what you see and read about the COVID-19 pandemic
- May 2, 2020, USA Today tried to debunk my April 7, 2020, article, “Vitamins C and D Finally Adopted as Coronavirus Treatment,” which has more than 814,600 views, without presenting any counterevidence
- The majority of mainstream media in the U.S. are owned, funded (through advertising) — and therefore easily controlled — by only a few powerful corporate entities and industries, some of which are overseas and may not even have American interests at heart
- Only 47% of American adults trust mainstream digital publishers to report accurate information about COVID-19. Still, 85% trust the CDC and 77% trust WHO, both of which have the same conflicts of interest as most mainstream media
- Both vitamin C and D have an enormous amount of evidence showing they provide important immune function benefits, and that your immune function is your front-line defense against all illness, including COVID-19
From Dr. Joseph Mercola
Since COVID-19 first entered the scene, exchange of ideas has basically been outlawed. By sharing my views and those from various experts throughout the pandemic on COVID treatments and the experimental COVID jabs, I became a main target of the White House, the political establishment and the global cabal.
Propaganda and pervasive censorship have been deployed to seize control over every part of your life, including your health, finances and food supply. The major media are key players and have been instrumental in creating and fueling fear.
I am republishing this article in its original form so that you can see how the progression unfolded.
Originally published: May 18, 2020
The fact that there is an information war going on is quite evident at this point. Mainstream media, supported by monopoly tech platforms like Google, YouTube, Facebook and Twitter, are going to great lengths to control the narrative of what you see and read about the COVID-19 pandemic.
Videos questioning the narrative — even when done by health professionals and scientists — are taken down faster than you can share them. Social media accounts of well-respected health professionals are being suppressed and removed. Twitter is even trialing a moderator tool that warns users when they’re about to post “harmful” language, although it’s unclear what the company might deem harmful.1
Fact-Checking at Its Worst
“Fact-checking” is also in overdrive, with journalists who are clueless about health and choose to side with the authoritarians writing articles “debunking” clear and provable facts without any counterevidence whatsoever.
Case in point: May 2, 2020, USA Today published “Fact Check: Vitamins C and D Are Not Used in ‘Conventional Treatment’ of Coronavirus,”2 an article aimed at debunking my April 7, 2020, article, “Vitamins C and D Finally Adopted as Coronavirus Treatment,” which has more than 816,000 views. USA Today writes, in part:3
“Mercola’s claim about vitamins and the coronavirus cites a New York Post article from March 24 that describes the use of vitamin C by Northwell Health, a New York hospital system, to treat patients with coronavirus.
Northwell spokesperson Jason Molinet confirmed to USA TODAY that ‘vitamin C was one of many therapies employed at the discretion of physicians in our health system.’
Molinet declined to answer follow-up questions about how widespread the use of vitamin C was, what the results of the treatment were and what studies or data Northwell relied on when deciding whether to use vitamin C as part of COVID-19 treatment. He declined to make a doctor available to speak about the treatment, saying, ‘That’s the extent of our statement on this.’
Our Ruling: False.
Though vitamin C is used, at least in one New York hospital system, to help treat some patients on a case-by-case basis, there is no known evidence to suggest it is effective.
Occasional use of vitamins C or D in COVID-19 treatment at the discretion of a patient and doctor is not the same as saying they are being adopted ‘in the conventional treatment’ of the coronavirus, as Mercola’s article says.”
This is beyond a shoddy “debunking” attempt. What does “adopted in conventional treatment” actually mean? The fact that vitamin C is being used in a conventional hospital setting to treat COVID-19 patients means it is in fact being adopted in conventional treatment.
I never stated or implied vitamin C is being used as “the standard of care” everywhere, but the fact is, it has been adopted as part of COVID-19 treatment by New York state’s largest hospital system.
My article also clearly states Northwell hospital system is using vitamin C “in conjunction with the antimalarial drug hydroxychloroquine and the antibiotic azithromycin.” I never stated or implied vitamin C is being used in isolation as the sole treatment, or that it could be (it probably shouldn’t).
So, essentially, USA Today confirmed my report, then slapped a “fake news” label on it after falsely asserting “there is no known evidence to suggest [vitamin C] is effective.”
My article, meanwhile, detailed the scientific evidence — with scientific references — underpinning the suggestion to use vitamin C and vitamin D to boost your immune system, which in turn can help protect against COVID-19, seeing how it protects against most other viral illnesses.
USA Today presents no such counterevidence. Instead, it cites an opinion expressed by the founder of QuackWatch.org in 2012 — eight years ago — and directs readers to information from the Centers for Disease Control and Prevention and the World Health Organization, which states “the only way to minimize the chances of contracting the virus is to take preventive steps such as social distancing ... frequent hand-washing and cleaning of often-used surfaces.”
Information Combat Is the New Warfare
Why do USA Today, CDC and WHO want the public to believe that there’s absolutely nothing they can do to protect themselves against SARS-CoV-2? Why do they want us to think our immune system is irrelevant when it comes to preventing and/or surviving COVID-19? Could it be because they want you to feel helpless enough to want a vaccine?
Rule 101 of debunking is that you have to present counterevidence. There’s clear evidence showing vitamin C’s usefulness against infectious disease, including sepsis, which is a major cause of death from COVID-19. If you’re going to claim that there’s “no known evidence to suggest vitamin C is effective,” then that means you have to produce studies showing vitamin C is useless against infections and sepsis.
So, why did USA Today not bother digging up those scientific references rather than quoting Quackwatch and directing readers to the CDC and WHO websites, where, again, no actual scientific evidence is cited? Could it be because their shoddy journalists are counting on people to not think critically?
Unfortunately, we’re bound to see more and more of this kind of irrational censoring of valuable health information as mainstream media pushes the WHO/CDC/Bill Gates narrative that our only hope for a return to normalcy is to vaccinate and digitally track, trace and surveil the global population.
In other words, their answer to the COVID-19 pandemic is the rapid rollout of a global totalitarian regime under which you can be placed in house arrest at any moment and be banned from travel, work, education, leisure and social activities simply because you’ve been infected or not infected/have or do not have antibodies/have or have not been vaccinated.
This strategy stands to make drug and tech companies untold billions of dollars, and the drug industry is undoubtedly a key player behind the media messages you see. The drug industry spent roughly $6 billon on drug ads to consumers in 2016,4,5 and drug ads (sometimes disguised as content through the use of something called advertorials) make up a fair share of the advertising dollars that media corporations depend on for their survival.
Download this Article Before it Disappears
Download PDFUSA Today Is Part of Media Monopoly
In November 2019, Gannett, the parent company of USA Today, merged with GateHouse Media, owned by New Media Investment Group.6,7,8 Together, they now form the largest media monopoly in the U.S., with more than 260 dailies under their umbrella.9
The management of this vast news network is done by Fortress Investment Group, a private equity firm, which in turn is owned by Tokyo’s SoftBank.10 According to CNBC,11 SoftBank’s CEO, the Japanese billionaire Masayoshi Son, also has “a wide network of relationships” in the tech industry and is said to be “one of the technology industry’s most influential investors.”
In 2018, Son funded EarthNow, a project involving 500 satellites equipped with machine learning technology to surveil the entire planet with real-time video. Another funder of this project was Bill Gates.12 (Incidentally, this project sounds like it could find a purpose in Gates’ proposed surveillance plan, and not be relegated to catching illegal fishing and tracking animal migration.)
My point, though, is this: The majority of mainstream media in the U.S. are owned, funded (through advertising) — and therefore easily controlled — by powerful corporate entities and industries, some of which are overseas and may not even have American interests at heart.
Media’s ties to Big Pharma and Big Tech run deep. Is it any wonder then that so often, so many news outlets use the same exact talking points on health, drugs, pesticides, GMOs and 5G, just to name a few? How is it that they’re using the identical language, as if they’re all reading and copying a single script?
Trust in Mainstream Media Is Rapidly Eroding
Fortunately, many are starting to see through the bias. The censorship has gotten so ridiculously blatant, it’s hard to miss. As a result, mainstream media are losing what little credibility they had left. Their machinations have simply become too obvious.
As of September 2019, American’s trust in mass media had dipped to 41%; only 13% trusted the media “a great deal.”13
March 19, 2020, Publishers Daily reported14 the results from a February 2020 Axios/Ipsos poll15 showing only 51% of American adults trust newspapers to provide them with accurate information about COVID-19 — the same ratio saying they track the pandemic “very closely.”
Only 47% trust mainstream digital publishers to report accurate information about COVID-19. Still, 85% trust the CDC and 77% trust WHO, both of which have the same conflicts of interest as most mainstream media.16
In the EU, the average net trust in the media as a whole is in the negative — minus 9% — when you include all forms, including radio, television, press, digital publishers and other online sources, including social media.17
Nutrition Is Essential to Protect Against Viral Illnesses
Regardless of what the mainstream media want you to think, many are starting to realize the truth, which is that both vitamin C and D have an enormous amount of evidence showing they provide important immune function benefits, and that your immune function is your front-line defense against all illness, including COVID-19.
As reported in the paper18 “Optimal Nutritional Status for a Well-Functioning Immune System Is an Important Factor to Protect Against Viral Infections,” published April 23, 2020:
“The role nutrition plays in supporting the immune system is well-established. A wealth of mechanistic and clinical data show that vitamins, including vitamins A, B6, B12, C, D, E, and folate; trace elements, including zinc, iron, selenium, magnesium, and copper; and the omega-3 fatty acids eicosapentaenoic acid and docosahexaenoic acid play important and complementary roles in supporting the immune system.
Inadequate intake and status of these nutrients are widespread, leading to a decrease in resistance to infections and as a consequence an increase in disease burden. Against this background the following conclusions are made:
(1) supplementation with the above micronutrients and omega-3 fatty acids is a safe, effective, and low-cost strategy to help support optimal immune function;
(2) supplementation above the Recommended Dietary Allowance (RDA), but within recommended upper safety limits, for specific nutrients such as vitamins C and D is warranted; and
(3) public health officials are encouraged to include nutritional strategies in their recommendations to improve public health.”
In related news, Finnish researchers have identified specific immune health-related genes that are regulated by vitamin D.19 In vitro tests show vitamin D targets genes that support immune function in response to acute infection, infection in general, and autoimmunity. According to the authors, “15 genes were identified as major mediators of the action of vitamin D in innate and adaptive immunity.”
Low Vitamin D Levels Linked to Increased COVID-19 Mortality
Irish researchers recently published an editorial20 highlighting the role of vitamin D deficiency in severe COVID-19 infections specifically. According to the authors:
“... the evidence supporting a protective effect of vitamin D against severe COVID‐19 disease is very suggestive, a substantial proportion of the population in the Northern Hemisphere will currently be vitamin D deficient, and supplements, for example, 1,000 international units (25 micrograms) per day are very safe.
It is time for governments to strengthen recommendations for vitamin D intake and supplementation, particularly when under lock‐down.”
You can learn more about this in “Vitamin D Level Is Directly Correlated to COVID-19 Outcome.” Similarly, a May 6, 2020, report21 published in Aging Clinical and Experimental Research (its prepublication featured in the Daily Mail May 122), found that countries with lower vitamin D levels have higher death rates from COVID-19. According to the authors:23
“The Seneca study showed a mean serum vitamin D level of 26 nmol/L in Spain, 28 nmol/L in Italy and 45 nmol/L in the Nordic countries, in older people. In Switzerland, mean vitamin D level is 23 nmol/L in nursing homes and in Italy 76% of women over 70 years of age have been found to have circulating levels below 30 nmol/L.
These are the countries with high number of cases of COVID-19 and the aging people is the group with the highest risk for morbidity and mortality with SARS-CoV2.”
In the preprint version24 of this paper, the authors concluded: “We believe that we can advise vitamin D supplementation to protect against SARS-CoV2 infection.” In the final version,25 they toned down the recommendation to: “We hypothesize that vitamin D may play a protective role for COVID-19.”
Gannett-owned USA Today is clearly, knowingly, publishing health news aimed at preventing people from effectively protecting themselves against severe COVID-19 infection. So, what’s their excuse for not sticking to scientifically verifiable facts?
- ‹ Previous
- 1
- 2
- Next ›
About
© 2025 Created by carol ann parisi.
Powered by
![]()