The Great Awakening-In God We Trust
FROM MERCOLA MEDICAL GASLIGHTING

STORY AT-A-GLANCE
- The medical industry has a vested interest in concealing injuries from its products
- A cruel but common method for accomplishing this is medical gaslighting
- Two of the most common diagnoses use to gaslight patients severely injured by the COVID-19 vaccines are "anxiety" and "functional neurologic disorder"
- Most doctors do not intend to gaslight their patients, but this behavior is an almost inevitable consequence of of their training and the modern practice of medicine. A patient understanding their perspective helps make it possible for doctors to see that patient's medical injuries
One of the classic ways an abuser controls their prey is to manipulate the environment so that the abused individual begins doubting their own observations regardless of what is occurring in front of them.
In the 1944 movie, Gaslight, this was accomplished by the villainous husband (played by Charles Boyer) adjusting the intake to gas-powered lights (causing them to flicker) and simultaneously denying that any change was occurring to his mentally abused wife (played by Ingrid Bergman). The term gaslighting originated from this classic movie.
In modern times, this is accomplished by having medical providers all echo the same message that a patient’s injury has nothing to do with the pharmaceutical (or other medical procedure in question). Most commonly, it instead is argued that the symptoms they are experiencing are due to pre-existing psychiatric issues the patient has (e.g., anxiety), which are treated with medications that often create additional issues.
Before we go any further, I want to emphasize just how miserable this is to go through as an injured patient. Imagine what it would be like if (due to the medical injury) the world you had previously known collapsed around you and every single person you trusted (including your friends and family who defer to the judgment of “experts”) told you that it was all in your head and you just needed psychiatric help. It’s a perfect recipe for going insane.
For example, let’s consider the recent experiences of Maddie De Garay in the pivotal Pfizer trial that was used to argue for the safety of the COVID-19 vaccines in the adolescent population:
Pfizer's trial only vaccinated 1,131 children so a single serious injury would have made the vaccine too dangerous.
— Pierre Kory, MD MPA (@PierreKory) January 11, 2023
Maddie's story shows just how far medicine will go to betray and gaslight patients who threaten its narrative. We may never know who else was swept under the rug. pic.twitter.com/4ONwty5Hu6
Note: This was clipped from episode 280 of the Highwire which we shortened (e.g., much of what she had to deal with in the hospital was cut out) so her story could reach a broader audience.
Although Maddie’s experience was atrocious, it was sadly not unique and many others had similar experiences in the COVID-19 vaccine trials. Similarly, I have heard many similar stories from other people who were harmed by the medical system.
Pharmaceuticals are inherently toxic. For example, most medications work by inhibiting enzymes (which are essential for life) and because of how interconnected the body is, this inhibition will create a variety of unintended consequences.
Similarly, most vaccinations function by making the immune system (often with the aid of toxins that help provoke that response) have an unnatural and narrowly focused response to a target substance.
The creation of this immune response unfortunately also often creates dysregulation within the immune system as this provocation can cause the immune system to be diverted away from attacking things it is supposed to address (e.g., microbes and cancers), while simultaneously triggering it to attack the body’s own tissue.
Since toxicity has always been inherent to the practice of allopathic (Western) medicine, the profession has gradually come up with a playbook to prevent its inevitable medical injuries from sabotaging business. This has essentially been accomplished by doing the following:
•Telling patients the adverse events they experienced either are not occurring or are unrelated to the toxic pharmaceutical.
•Developing an elaborate scientific apparatus that provides evidence refuting the link between these injuries and pharmaceuticals on the market, while concurrently training the population to defer to the scientific consensus rather than trusting their own observations.
•Making competing forms of medicine that lack a similar degree of inherent toxicity illegal, therefore making the only choice within the existing medical monopoly be a toxic form of medicine (similarly consider how allopathic medicine is always considered to be the best form of medicine every other approach must find a way to measure up to).
This is also why we have the doctrine in allopathic medicine that every treatment has risks and the treatments are chosen because its benefits outweigh its risk (as opposed to just exploring systems of medicine without those risks).
All of this in turn results in the tragic phenomenon known as medical gaslighting, or as some like to put it “allopathic medicine gaslights you to death.”
Why Can’t Doctors Diagnose Medical Injuries
I have found numerous documented examples of medical gaslighting stretching back to the late 1700s and in each case, typically only a minority of the medical profession is willing to acknowledge the injuries that are occurring could be linked to their pharmaceuticals.
At the same time, it’s rare for me to meet doctors I consider to be evil; on the contrary, most tend to be remarkably intelligent and well-intentioned individuals who genuinely want the best for their patients.
At this point, I believe medical gaslighting is a natural consequence of our training. Since the therapeutic toolbox of allopathic medicine is quite limited, most doctors cannot practice their craft without administering unsafe pharmaceuticals to their patients, and thus for the sake of their self-identity, they must fully believe in their pharmaceuticals (this subject was discussed further here).
It is an enormous personal investment to become a physician and it is extremely difficult for someone who goes through that to acknowledge that much of what they learned is highly questionable.
Similarly, no well-intentioned doctor wants to harm a patient, and since they often do, the reflexive psychological coping mechanism is to deny the possibility of each injury that occurs (discussed further here).
This first dawned on me at the start of my medical education when one of our professors inserted a tirade against anti-vaxxers into his lecture and concluded his argument with “… and just think about it. Do you really think pediatricians would vaccinate their patients if they thought vaccines could harm them?”
Although widespread denial of the harms that Allopathy causes likely explains some of my profession’s predilection for gaslighting, I do not believe it is the primary issue. Instead, I believe it is a result of the training doctors receive making them unable to recognize medical injuries.
The Origins of Medical Blindness
Because the human body is immensely complex, humans in every era face significant difficulties in being present to everything that is occurring within a human being. Most medical systems address this challenge by creating diagnostic models which simplify the immense complexity present in each patient down to the key things that must be focused upon to positively affect patient wellbeing.
The downside to this approach is that there will always be things in each patient that lie outside the diagnostic model being used to evaluate them. When this happens, those things understandably will not be recognized (unless the medical practitioner innately can perceive a complexity that transcends the limitations of their diagnostic model, something the majority of the population is not capable of).
In the case of allopathic medicine, we are taught a diagnostic model that is excellent for identifying many things (particularly indications for prescribing pharmaceutical drugs). However, our model also fails to notice many other things which are critical for health and wellness.
For example, much of medicine is taught by having a series of lists to memorize that are plugged into linear algorithms. Because this requires breaking many complex subjects into a binary “yes” or “no,” many important things that lie between these two polarities get lost in translation.
This is the easiest to illustrate with the nervous system (but the issue is by no means exclusive to it). When evaluating it, one of the things we are all taught to do is quickly check if the twelve cranial nerves are functioning normally (e.g., can you swallow, make a smile, or follow a finger with your eyes).
Frequently, although the cranial nerves are “generally normal” they will have some difficulty firing (e.g., at some point in the motion arc as the eyes travel side to side, they will jump instead of moving smoothly). These “minor” deficits often have a significant impact on a patient’s quality of life, but in most cases (except when evaluated by certain neurologists or neurosurgeons), the function of those nerves will be noted as normal and ignored.
One of the most common signs of a vaccine injury is a subtle cranial nerve dysfunction (discussed further here). While these are very easy to recognize if you are trained to look for them, that training does not exist within allopathic medicine, and as a result, most physicians simply cannot see the large number of vaccine injuries occurring around them.

Download this Article Before it Disappears
Download PDFSimplifying Illness
The cranial nerve example unfortunately is only one of many areas where a complex presentation of symptoms is simplified into a box that excludes an inconvenient diagnosis from ever being recognized. Another common way this boxing occurs is when an authoritative diagnosis is used to define a complex phenomenon without actually stating what it is.
For example, many disorders in medicine are simply symptoms written in Latin. Dermatitis quite literally translates to “inflammation of the skin,” and in most cases is simply treated with a cream that suppresses that inflammation.
Conversely, in many other medical systems, inflammation of the skin is recognized as an important sign of something being awry in the body, and the exact character and location of the inflammation are focused upon to identify and address the root cause of that inflammation (to some extent this is recognized in dermatology, but even there it occurs nowhere to the degree that it should).
Similarly, “migraine” headaches, although not exactly Latin, falls into a similar boat. While many things can cause migraines (e.g., they are very frequent after COVID-19 vaccine injuries) their cause is rarely focused upon, and instead, the standard medical approach is to throw pharmaceuticals at them until something improves the headache.
In my medical practice, I frequently treat migraines. In these patients, I find over and over that they have seen numerous doctors (including highly regarded specialists). Despite this, it is very rare anyone they saw was able to recognize the diagnostic signs or aspects of their history that point to the root actual cause of their headaches, and thus, not surprising that they will simply be prescribed more and more medications in the hope one will work.
Framing the Iatrogenic Debate
Iatrogenesis is the term for any type of illness or medical complication resulting from a bad reaction to medical care (e.g., a complication from a surgery or a pharmaceutical). A common pattern I’ve observed for decades is everyone denying a particular iatrogenic complication exists (e.g., “there is no evidence”), and then once overwhelming evidence exists that it does, it will be acknowledged.
Once this happens, the harm from the drug will be reframed so that only the accepted harm can be bad and an underlying assumption is created that nothing else is a possible complication.
For example, fluoroquinolones (e.g., Cipro) are fairly toxic antibiotics that can severely harm people and are frequently given for many minor infections (e.g., urinary tract infections) where their corresponding toxicity is simply not justified.
In medical school, everyone learns that a tendon rupture (something unique and hard to ignore) is a side effect of these drugs, and as a result, when doctors evaluate for harms, they will look for that but not be able to recognize most of the other well-documented complications from them.
My favorite recent example of this reframing occurred with the J&J COVID-19 vaccine. At the start of Operation Warp Speed, I hypothesized that a major goal was to get mRNA technology onto the market since it held the promise of trillions of dollars in future revenue for the pharmaceutical industry (but since there were safety challenges with it, nothing short of an "emergency" would be able to break the barrier to human testing).
Because of this, I suspected that once vaccine safety concerns emerged, a non-mRNA COVID-19 vaccine would be thrown under the bus to make the mRNA technology look “safe.” This is what then happened with the J&J vaccine when six cases of an extremely unusual blood clot being linked to that vaccine caused the FDA and CDC to pause its administration for 11 days.
By doing so, it created the perception the FDA was monitoring for vaccine side effects with a fine-tooth comb and was willing to pull the vaccine if it caused a rare side effect in a very small number of people.
Nothing could be further from the truth as the mRNA vaccines have caused far more blood clots than the J&J vaccine. Similarly, investigation after investigation shows the FDA is ignoring the endless deluge of red flags from the COVID-19 vaccines.
Unfortunately, this ploy worked, and in the odd instances where I hear a doctor willing to debate the safety of the vaccines, one of the most common arguments they still utilize is that if the FDA was willing to temporarily pause J&J after six blood clots, there is no possible way a larger unaddressed problem exists with the mRNA vaccines.
Psychiatric Complications and Iatrogenic Injuries
As the above points have shown, a variety of factors work against doctors being able to recognize the presence of medical injuries. The question then becomes, how will the injuries that inevitably occur be explained?
As you might imagine, the default strategy is to fold the injury into an amorphous diagnosis which (instead of allopathic medicine) can take the blame for the medical injury and then put that label on everyone with the injury. Typically this is done with psychiatric diagnoses, but recently COVID-19 infections have also been appointed to that role (both of these diagnoses were used to gaslight patients in the clinical trials for those vaccines).
The earliest references to this gaslighting I have found were at the time of Freud, where his new model of psychoanalysis was used to explain the complex symptoms observed within patients doctors otherwise had difficulty making sense of. However, as detailed in The Age of Autism: Mercury, Medicine, and a Man-Made Epidemic, an outside evaluation of Freud’s case studies suggests those patients’ problems actually arose from mercury poisoning.
Mercury, despite being extremely toxic, was used by the medical profession for centuries (and to some extent still is). Frequently, individuals with mercury poisoning would develop a wide array of complex diseases which included neurological and psychiatric complications (which like many other conditions were often attributed to “female hysteria”).
Freud’s message that these complications were the fault of the patient (e.g., as a result of unresolved sexual desires) rather than the physician was an immensely appealing message to the medical profession, and as a result, became the party line.
Ever since this time there has been a systemic failure to recognize that neurologic damage can produce psychiatric symptoms. Instead, neurologic symptoms are viewed as a manifestation of a pre-existing psychological illness that must be treated with psychological counseling and psychiatric medications.
One of the best examples of this issue is “Functional Neurological Disorder” (FND) which recognizes that something is wrong with the brain, but since no explanation can be found, it is assumed to have been due to pre-existing psychiatric conditions.
If you review the National Institute of Health’s description of FND, you will see that the above description is no exaggeration, and it is extremely sad to hear about the experiences vaccine-injured patients go through since FND is one of the most common diagnoses they receive.
When I look at FND cases, the cause of the disorder (e.g., seizures) can frequently be found, but since neurologists (including friends of mine) do not want to consider the actual cause, the tests needed to diagnose it are often not ordered or even known about by the doctors attending to the patient.
If you review Maddie’s story, you will note that this is also exactly what happened to her and her permanent paralysis from the vaccine was labeled as FND resulting from a psychiatric condition. Because of this gaslighting, she was not able to get appropriate care when her neurological reaction to the vaccine was occurring (that would have prevented permanent disability).
I believe this occurred because the chief investigator was fully aware that a severe neurologic reaction to a single participant would have made the vaccine too dangerous for children to take, so he decided to gaslight Maddie so her injury would not need to end up in the trial. Sadder still, Maddie’s experiences were not unique, and their experiences that indicate systemic fraud in the vaccine trials were detailed here.
Another common symptom doctors place the blame for medical injuries on is “anxiety.” The two major problems with this process are:
- Failing to recognize that having a life-changing injury will normally create distress, and similarly failing to recognize that being collectively gaslighted by medical providers is not good for anyone’s mental health.
- Pharmaceutical injuries frequently cause tissue damage that will trigger anxiety.
Sadly, very few doctors recognize that damage to the nervous system (which is a common toxicity of pharmaceuticals) can also create psychiatric disturbances. Instead, they only can recognize that psychiatric distress can often worsen neurologic symptoms, but do so without also realizing that it is much rarer for psychiatric distress to be the originating cause of a neurologic issue.
Similarly, many common psychiatric disorders have organic causes (e.g., chronic undiagnosed infections, traumatic brain injuries, or nutritional and metabolic deficiencies). However, in most cases, psychiatrists prescribe medications based on the symptoms a patient presents with (e.g., you are depressed so you need Prozac) rather than looking at the underlying cause.
I believe this is because doing the former pays well but the latter typically does not and is not emphasized in a psychiatrist’s training.
In addition to neurological damage frequently creating psychiatric complications (e.g., vagal dysfunction creating anxiety), damage to other organ systems can as well (Chinese medicine does an excellent job of mapping these correlations out). One of the best examples I have seen with the COVID-19 vaccines relates to the heart and I have had variations of the following conversations multiple times since 2021:
Friend: I have been having severe anxiety attacks since I got the vaccine. My heart starts beating rapidly, and I start to have pain in my chest. I never had this problem before, but now everything makes me anxious and it’s so hard for me to be calm.
Me: You should get your heart looked at.
Friend: What do you mean? Everyone told me it was anxiety due to stress.
Me: Trust me, you need to get your heart looked at.
(Time passes)
Friend: How did you know I had myocarditis?
Damage to the heart (or the vagus nerve) will often create an irregular heart rate and chest pain, and these palpitations often provoke anxiety. Unfortunately, since these symptoms are also triggered by anxiety, when they are observed, doctors will often default to a diagnosis of anxiety and look no further.
Conclusion
There are essentially two models of medical practice which are followed:
- The paternalistic model (where you are expected to unquestioningly trust and comply with everything the doctor tells you).
- The collaborative model where the physician is your partner in working towards health.
Although the paternalistic model was the standard for most of allopathic medicine’s history, in recent times, there has been a push for the collaborative model. Presently, many patients are seeking out collaborative physicians (especially since system doctors have to spend so much time going through checklists that there is little time for actual engagement with their patients), and the market is economically rewarding physicians who are making this change.
A key misconception much of the public holds about doctors is that we are infallible beings (which is a key justification for the paternalistic model). In reality, once you peer behind the lab coat, we struggle with many of the same issues you all do too. Being able to genuinely recognize this and respectfully treat the physician you see as a fellow human being is one of the most effective strategies for initiating a collaborative doctor-patient relationship.
Although doctors sometimes gaslight injured patients for self-serving reasons (e.g., to protect Pfizer’s vaccine in its clinical trials or under the misguided belief it will protect a doctor from a lawsuit), I believe the majority of cases occur because the doctors simply cannot see the injury occurred. As a result, these doctors believe they are doing the best for the patient when in reality they are just gaslighting them.
One of the largest issues in our modern era is how disconnected we have become from ourselves and others. Within the doctor-patient relationship, this disconnection makes it much less likely a physician will be able to recognize what is happening in a patient (e.g., a medical injury) or feel compelled to go to bat for them while every other healthcare provider is gaslighting them.
When people ask me for their best options to avoid being gaslighted, I thus suggest pursuing one of the following options:
1)See a physician who you pay directly (rather than one who takes insurance). This business model matters because it forces the doctor to have a collaborative doctor-patient relationship and stay in business (no one will pay to see them if they just get gaslit). I am a big believer in the statement “you get what you pay for” and if only see system doctors who base their practice around insurance payments, you often do not get a good outcome.
For example, I had a patient recently who I felt exemplified this issue. He had what I felt was a relatively straightforward problem that had significantly impacted his life for 25 years. When I reviewed his history, he told me he had seen a dozen (insurance-taking) doctors, many of whom promised they could fix the problems with elaborate procedures from their specialty (all of which did nothing or made his issue worse).
What was striking about his story was that only one of them had ever even performed an extensive evaluation (e.g., talking with him about the history of his disease) to try to figure out what was causing the problem.
2)However, while seeing a private-pay physician often is an excellent investment, many patients simply cannot afford to do so. In this case, the ideal scenario is to find an insurance-taking physician through word of mouth who has earned a reputation for forging collaborative doctor-patient relationships. Unfortunately, these recommendations are hard to come across and typically these doctors will have full practices that are hard to get into.
3)The third (and often the only available option is to take the initiative to forge a collaborative relationship with the doctor through having a respectful demeanor where you treat the doctor as a fellow human being rather than “the doctor.”
In general, this approach will be the most effective on doctors who recently completed their medical training (everyone becomes more rigid with age, plus their practices are not yet full), and in medical settings where the doctors get longer per visit (you can’t really build a collaborative relationship in 10-15 minutes).
Regardless of the option you choose, it is also often important to provide the documentation to support the occurrence of your medical injury. This includes records establishing a timeline of the injury following the medical therapy and scientific literature substantiating the link between the two.
Physicians in turn (especially younger ones) will be the most receptive to considering this link if it is presented in a composed and thoughtful way rather than a confrontational manner, because like every other human they tend to become defensive. Given how upsetting the process of being gaslighted is, maintaining this demeanor can be extremely challenging.
Sadly though, it is necessary because doctors are trained to see these injuries as being psychological in nature, and a patient expressing their completely justifiable feelings about the situation will often feed into the doctor’s erroneous perceptions about the patient’s mental health.
About the Author
A Midwestern Doctor (AMD) is a board-certified physician from the Midwest and a longtime reader of Mercola.com. To find more of AMD's work, be sure to check out The Forgotten Side of Medicine on Substack.
Views: 39
Comments are closed for this blog post
-
Comment by carol ann parisi on February 20, 2023 at 4:40pm
-
The situation in Ohio is absolutely tragic and how they’re downplaying the danger of what’s going on.
The belief that “a little bit is okay” is patently false, according to the research of renowned functional medicine practitioner Dr. Bryan Walsh.
HERE is a quick guide of what you may have been exposed to (or may be exposed to as these chemicals spread through the air and Ohio River Basin)...
Here it is - Copied from them:
Exposure List - What We Know:
Vinyl Chloride
- Smell: “mild, sweet odor.”
- Vinyl chloride is used to make polyvinyl chloride, better known as PVC, which goes into plastic pipes, cable coatings, and packaging materials.
- Can cause dizziness and disorientation.
- Chronic exposure may lead to liver cancer.
Ethylene glycol monobutyl ether
- Smell: Almost odorless.
- Used in varnishes, paint thinners, agricultural chemicals, and industrial and household cleaners.
- May cause irritation of the nose and eyes, headaches and vomiting.
Butyl acrylate
- Smell: Fruit, strong odor.
- A clear, colorless liquid with a strong odor— that is used for making paints, caulks and adhesives.
- It can cause breathing difficulties and irritation of the eyes and skin.
Ethylhexyl acrylate
- Smell: “Pleasant odor.”
- Used for making paints and plastics.
- Symptoms: Can irritate the skin, eyes and respiratory tract.
Isobutylene
- Smell: “Sweet, gasoline odor.”
- Used in the production of isooctane, a component of some gasolines.
- Breathing it in can cause dizziness and drowsiness.
- Smell: “mild, sweet odor.”
-
-
-
-
DIABOLICAL: WHO considers COVID shots “one of the most successful and cost-effective public health interventions”
by: February 18, 2023
 (NaturalHealth365) If you were to believe everything presented during the nightly news, you would believe the World Health Organization (WHO) – which considers all immunizations, including the COVID injection, to be infallible. The widely accepted narrative is that public health interventions are economically efficient and a net positive for the human condition. Yet, we know, this narrative is a pure lie, given the fact that the jab has caused hundreds of thousands of deaths.
(NaturalHealth365) If you were to believe everything presented during the nightly news, you would believe the World Health Organization (WHO) – which considers all immunizations, including the COVID injection, to be infallible. The widely accepted narrative is that public health interventions are economically efficient and a net positive for the human condition. Yet, we know, this narrative is a pure lie, given the fact that the jab has caused hundreds of thousands of deaths.As soon as you embrace that idea that you’ve been lied to, you’ll begin to question the WHO’s endgame. How can a supposedly charitable organization turn a blind eye to the negative health consequences of the Covid shots? Critical thinkers rightfully question whether the COVID shots are a means to a nefarious end that will never be fully revealed to the masses.
WHO ignores immense harm inflicted by COVID shots and declares “success”
Read through the news releases and announcements made by the WHO’s public relations department, and you’ll find it is chock-full of propaganda presented in supposed fact form. Spend half an hour on the WHO website, and you’ll discover half-truths and even some bald-faced lies, many of which have been debunked in neglected corners of the web.
As an example, the WHO narrative states receiving the COVID shot has the potential to be lifesaving. The organization’s representatives insist coronavirus injections protect against sickness and even death. Furthermore, the WHO narrative highlights how the shot reduces the chances of passing the virus to friends, family, coworkers, and others you cross paths with.
The WHO wants you to blindly accept that the decision to get injected is a public service that will eventually halt the spread of this deadly virus. If you are still in the midst of waking up, shift your attention to alternative sources of news across the web. You’ll find that the Covid shots do not protect against infection nor prevent transmission.
How the COVID shots decimate humanity, as we know it
If the American mainstream media expanded its source material in the spirit of objectivity, it would reference the recent report out of the UK revealing how the COVID shot is deadly. The UK government’s shocking admission of how the injection causes death directly conflicts with the WHO’s statements to the contrary.
If you were to force officials from the UK to sit in a room with representatives from WHO to discuss the safety and efficacy of the Covid shots, you would witness quite the cognitive dissonance play out. Representatives from the UK would highlight how mortality rates in uninjected age cohorts are lower than those in all those people that received the Covid shots. Furthermore, truth-tellers from the UK would also point out how the gap in death rates between the people that accepted the shots and those that did not get injected expand with each passing month.
The pressing question is why our federal government refuses to acknowledge such truths, choosing to push a false narrative. Continue to ask questions, and you’ll make your way to the truth.
Unfortunately, we live in a world where corporate monetary donations (especially from the pharmaceutical industry) to our so-called political “leaders” has corrupted our government at the federal and state levels. We need to replace them with better quality leaders that truly protect the public.
-
-
The New Abnormal: The Rise of the Biomedical Security State- Interv...
The New Abnormal: The Rise of the Biomedical Security State- Interv...
The New Abnormal: The Rise of the Biomedical Security State- Interv...
The New Abnormal: The Rise of the Biomedical Security State- Interv...
The New Abnormal: The Rise of the Biomedical Security State- Interv...
-
-
Eye Drops Linked to Antibiotic-Resistant Bacterial Infection
Analysis by Dr. Joseph MercolaFact Checked
- February 18, 2023

STORY AT-A-GLANCE
- January 20, 2023, the CDC announced an investigation into a multistate cluster of infections from May 17, 2022, to January 19, 2023, caused by Carbapenem-resistant Pseudomonas aeruginosa associated with artificial tears
- The infection was identified in 50 patients across 11 states, causing one death and at least three people to go blind in one eye
- Antibiotic resistance has been rising since the discovery of penicillin and now contributes to 4.95 million deaths worldwide each year; without change, consumption of antibiotics is estimated to increase by 200% by 2030
- Dry eye can be temporary from environmental factors like dry air or exposure to smoke, or it can be chronic. Data show optimizing vitamin D and omega-3 levels and using curcumin can all help ameliorate the symptoms of dry eye
Aging may be inevitable, but many age-related problems do not need to be. For example, your vision is largely dependent on your lifestyle. Your eyes, like many other organ systems, require appropriate nutrients throughout the years to ensure you maintain good eyesight and lower the potential of dry eye.
In late January 2023, a brand of eye drops marketed for dry eyes was connected to drug-resistant bacterial infections.1 Eye lubricant drops are marketed to support your tears. Your eyes need tears to keep them wet, smooth and to help focus light so you can see clearly. Your body uses tears to protect the eye from infections and foreign body irritations, like dust and dirt.
There are three different layers of fluid in your tears. Each layer is produced differently and performs a different function. The outer layer is an oily surface that keeps the watery layer from drying too quickly. It also makes the surface of the eyes smooth. The middle layer is watery and helps nourish the eye tissue and keep the eyes moist. The innermost layer of fluid is mucus.
This helps the watery layer stick to the surface of the eye and remain in place. Together these three layers are called the tear film. Inside the tear film are factors that help suppress inflammation in the eye, promote wound healing and defend against infection.2
You also have three different types of tears. Basil tears are the type just described that always stay in your eyes to help lubricate them and protect your cornea. Reflex tears are produced when an irritant is in your eye, such as a foreign body. These tears are released in large amounts to help flush out the foreign body and fight bacteria.
Finally, you produce emotional tears in response to sadness, joy and fear. According to the American Academy of Ophthalmology,3 some scientists propose emotional tears contain hormones that are not found in other types of tears. They hypothesize the stress hormones released in emotional tears may help regulate the body.
EzriCare Artificial Tears Linked to Infection
January 20, 2023, the CDC4 announced they were investigating a multistate cluster of infections caused by Carbapenem-resistant Pseudomonas aeruginosa that appeared to be associated with EzriCare Artificial Tears. The CDC stated they had identified 56 isolates from 50 patients across 11 states from May 17, 2022, to January 19, 2023.
The common exposure among the patients was the use of EzriCare Artificial Tears, which is a preservative-free product sold in a multidose bottle. The bacteria were isolated from several areas of the body, including cultures of the cornea, sputum, urine, blood and rectal swabs. January 24, 2023, EzriCare5 announced they had not received consumer complaints or reports of adverse events.
At that point, they also claimed to have “not received communication from any regulatory agency providing any outcomes or details to EzriCare about the ongoing investigation.”6 February 1, 2023, the company announced they received notice of the investigation, had stopped distribution and began contacting customers to advise them to discontinue use.
According to EzriCare, the artificial tears product is manufactured by Global Pharma Healthcare Pvt Limited in India and imported by ARU Pharma Inc. EzriCare places its label on the bottles and markets them to their customers. The company's understanding is that the same product is also marketed under other brand names.
According to the CDC, as of January 20, 2023, there has been one death when pseudomonas entered the bloodstream. According to Fox News,7 there were 11 reported cases of eye infections and at least three people who became blind in one eye from the infection.
According to the CDC,8 pseudomonas aeruginosa is one type of pseudomonas that causes hospital-acquired infections. It is commonly found in the soil and water. Pseudomonas aeruginosa has become multidrug resistant and in 2017 caused an estimated 32,600 hospital-acquired infections and an estimated 2,700 deaths.
Antibacterial Resistance on the Rise
Interestingly, the first clinical use of antibiotics was Pyocyanase,9 which was extracted from pseudomonas aeruginosa and used in hospitals in the 1890s. Not long after the introduction of penicillin, doctors began noticing antibiotic resistance in bacteria that had once quickly succumbed to treatment. And the problem continues to grow.
In 2013, the CDC10 published the first Antibiotic Resistant Threats Report to highlight the danger of antimicrobial resistance and underscore the threat to human health. The 2022 report found much of the progress had been lost, in large part to the overuse of antibiotics during the COVID-19 viral pandemic.
Antibiotic-resistant pathogens are conservatively estimated to cause at least 2.8 million infections annually in the U.S.11 and lead to 35,000 deaths each year. Globally, data from a study12 published in February 2022, show there are 4.95 million deaths associated with antibiotic-resistant infection and 1.27 million directly attributable to them.
Even as the challenge of antibiotic resistance was better understood, global consumption of the drugs rose by 65% between 2000 and 2015,13 driven by low- and middle-income countries where the drugs are often available without a prescription, which increases the risk for potential abuse. Antibiotics are routinely used to promote growth in livestock,14 and use accounts for about 80% of all antibiotics.15
The danger associated with giving livestock antibiotics is that it changes their gut microbiome, which is in part how they promote unnatural growth in the animal. However, some of those gut bacteria become antibiotic resistant. These can either be passed into the environment through the animal’s manure or may contaminate the meat during slaughter or processing.
The problems with antibiotic resistance need to be addressed through public policy. Yet, our individual choices influence personal risk. You can help lower your risk of contracting and or spreading a drug-resistant infection using some of the following strategies.
•Practice infection prevention, with a focus on naturally strengthening your immune system. Foundational strategies include avoiding sugars, processed foods and grains, stress reduction and optimizing your sleep and vitamin D level. Adding in traditionally fermented and cultured foods helps optimize your microbiome. Properly wash your hands with warm water and plain soap, to prevent the spread of bacteria.
•Limit your exposure to antibiotics — Keep in mind that antibiotics do not work for viral infections. Avoid antibiotics in food by purchasing organic or biodynamic grass fed meats and animal products and organically grown fruits and vegetables. Avoid antibacterial soaps, hand sanitizers and wipes, as these promote antibiotic resistance by allowing the strongest bacteria to survive and thrive in your home.
•Take commonsense precautions in the kitchen — Kitchens are notorious breeding grounds for disease-causing bacteria. To avoid cross-contamination between foods in your kitchen, adhere to the following recommendations:
◦Use a designated cutting board, preferably wood, not plastic, for raw meat and poultry, and never use this board for other food preparation. Color coding your cutting boards is a simple way to distinguish between them.
◦Sanitize your cutting board with hot water and detergent. For an inexpensive, safe and effective kitchen counter and cutting board sanitizer, use 3% hydrogen peroxide and vinegar. Keep each liquid in a separate spray bottle, and then spray the surface with one, followed by the other, and wipe off.
◦Coconut oil can also be used to clean, treat and sanitize your wooden cutting boards. It's loaded with lauric acid with potent antimicrobial actions. The fats will also help condition the wood.
Download this Article Before it Disappears
Download PDFWhat Is ‘Dry Eye’?
Another step to lowering your risk of infection is to reduce your dependence on over-the-counter products, such as artificial tears. Artificial tears or eye lubricants are used to help ease the symptoms of dry eye syndrome. This happens when the eye is unable to produce enough tears to maintain a healthy eye environment. The incidence of dry eye increases with age and may be related to hormonal changes.16
Other environmental factors that trigger temporary symptoms of dry eye include wearing contact lenses, a dry indoor environment, smoking or secondhand smoke exposure, or cold and allergy medications. In some cases, chronic dry eye may be caused by a nutritional deficiency, or damage to the tear gland. The most common cause of tear gland damage is Sjögren’s Syndrome, which is a systemic autoimmune, rheumatic disease that affects the whole body.
Symptoms of dry eye include blurred vision, sensitivity to light, burning, itching or redness in the eye, or a scratchy feeling. Depending on the type or cause of the condition, an ophthalmologist may prescribe over-the-counter eye drops, prescription medications, tear duct plugs or surgery.
The American Optometric Association17 recommends several steps to prevent temporary dry eye. This includes blinking regularly when you're staring at a computer screen for a long time, wearing sunglasses to reduce exposure to the sun and dry winds and increasing the humidity at work and home. Dehydration and a lack of sleep can also contribute to temporary symptoms of dry eye.
Tips to Treat Dry Eye Naturally
While it may seem easier to grab a bottle of artificial tears, the long-term solution is to make slight changes in your lifestyle habits and nutritional intake to help offset the condition. Your tears are made in part with water, so it makes sense to stay hydrated. Dehydration also leads to you feeling tired, grumpy and sick, and accelerates biological aging.
It's not necessary to count how many glasses of water you drink each day. Two indicators you need fluid are your thirst and the color of your urine. Thirst helps ensure your needs are met on a day-to-day basis. The color of your urine can also be used as a guide. While your urine color can be influenced by medication or supplements, overall, if it's a deep dark yellow, you are likely not drinking enough water.
Adequate hydration is indicated by pale, straw-colored or light-yellow urine. Most healthy individuals urinate on average seven to eight times each day. If you aren't urinating at least every two to three hours while you're awake, it may indicate that you're not drinking enough.
Optimizing your vitamin D levels also protects against dry eye syndromes. A 2015 study18 called it “more than an incidental association” and concluded that dry eye and impaired tear function in patients with a vitamin D deficiency indicate it plays a protective role.
As I've discussed in the past optimizing vitamin D levels affects many bodily systems including reducing your risk of infectious disease,19 cardiovascular disease20 and autoimmune diseases21 to name just three.
Regular sensible sun exposure is the best way to optimize your vitamin D status, but many need an oral vitamin D3 supplement during the winter months. The only way to gauge whether you need a supplement and how much to take, is to test your vitamin D level, ideally twice a year. This is particularly important if you're pregnant, planning to become pregnant, or if you have cancer.
The optimal level is between 60 nanograms per milliliter (ng/mL) and 80 ng/mL with 40 ng/mL being a low cutoff point for sufficiency to prevent a wide range of diseases. GrassrootsHealth22 makes testing easy by offering an inexpensive vitamin D3 testing kit and an online vitamin D3 calculator you can use to estimate the dosage once you know your current serum level.
Another nutritional supplement that is effective in preventing and supporting eye health is omega-3 fatty acids. This is a recommendation from the American Optometric Association23 and a survey24 of 206 optometrists in Australia and New Zealand. In that survey, 78% recommended omega-3-rich foods or supplements for dry eye disease and 79% said they recommended their patients consume omega-3 fats to improve their eye health.
Although fish oil is a well-known source, it has several drawbacks, including the lack of phospholipids. Omega-3 fats DHA and EPA are water insoluble and thus must be packaged into lipoprotein vehicles such as phospholipids. This is primarily why krill oil bioavailability is so much higher than fish oil since the DHA and EPA in fish oil are bound to triglycerides. Marine sources high in omega-3 and low in environmental pollutants include:
- Wild Alaskan salmon
- Small fatty, cold-water fish such as herring, sardines and anchovies
- Fish roe
- Krill oil
Finally, data also show that curcumin has a beneficial effect on several ocular diseases, including dry eye syndrome. In a 2014 paper,25 the researchers noted the beneficial effects on dry eye as did researchers in 201926 and 2020.27
It is a potent antioxidant28 and boosts the function of your own antioxidant enzymes.29 Overall, curcumin appears to be powerful, cost-effective and has a low toxicity profile. As such, it could be a valuable supplement. It is also worth noting the beneficial impact on pathways that help reverse insulin resistance, metabolic syndrome and obesity.30,31
I believe curcumin is a valuable nutritional addition worthy of consideration for all-around good health since inflammation drives so many different disease processes.
-
-
V-Safe Part 7: CDC Deceived the Public With Limited Release of V-Sa...
Seventh part of an incredible story that shows just how broken our public “health” apparatus is: very, very broken.

If you have not already read Parts 1 through 6 of the v-safe saga, please read those first!
Did CDC cherry-pick v-safe data over the last two years? Yes!
This is where it gets even more interesting. The CDC did release some check-the-box v-safe data in published studies prior to being forced to release all the v-safe check-the-box data by ICAN’s legal action.
The consistent game that the CDC played in these studies is to only publish the data concerning health impacts for the first week after the shot! (As a reminder, “health impacts” in v-safe means sought medical care, missed school/work, or unable to perform normal daily activities.)
CDC released study after study claiming the vaccine was safe but only included the health impact data for the first week after the shot. Only the first week.
Remember, the CDC specifically chose to capture health impact information at 1, 2, 3, 4, 5, and 6 weeks after the shot, and then at 3, 6 and 12 months after the shot. And the CDC knows, as discussed below, these vaccines can cause harm well after the first week after injection. Nonetheless, despite a diligent search, we could not identify a single study or report from the CDC which released health impact data further out than the first week after receiving the shot.
Why did the CDC not release this information? Did the CDC not like what that data had to show after the first week? Did it not fit in with its policy objective of promoting the shot to every American? Would it, after zealously promoting the vaccine and claiming it is safe, have hurt the CDC’s reputation?
Just to make sure context is not lost, the 7.7% figure of unique v-safe users who sought medical care was derived by analyzing all instances of medical care that CDC designed v-safe to capture. CDC chose to track the need for medical care at certain intervals. To avoid cherry-picking, 7.7% was derived by simply looked at the percentage of unique individuals using v-safe who reported seeking medical care.
If the CDC didn’t think it was relevant to capture or assess users seeking medical care after 7 days, why ask if a user sought medical care at 14 days? Or at 21 days? Or at 28 days? Or at 35 days? Or at 42 days?
But yet, here is an example of the data from v-safe that the CDC published in its study (deceitfully) entitled Safety monitoring of mRNA vaccines administered during the initial ... on March 7, 2022, which only included data from the first 7 days after the shot:

As you will see in the “Reported medical care” row, CDC reported that between .8% and 1% reported needing medical care in the first week after the shot, depending on dose and brand.
Putting aside that this rate should not have been comforting, CDC is actively seeking to have the public rely on this study to prove the Covid-19 vaccines are safe, in order to increase vaccine uptake, knowing that it is at best misleading.
You can see this same pattern repeated in study after study at the end of this article.
CDC Knows Vaccine Harms Arise Weeks After Vaccination
CDC is being deceitful because it knows harms from these vaccines can happen after 7 days. Indeed, as those who litigate vaccine injury claims all know, it typically takes at least a week, and often longer, for various vaccine harms to manifest. For example, autoimmune issues. As another example, consider myocarditis after Covid-19 vaccination – this often arises at least a week after vaccination as seen in figure 1 of this study showing the incidence of myocarditis during a 42 day period after receipt of the first dose of Pfizer’s Covid-19 vaccine. Similarly, TTS, which can be caused by the Covid-19 vaccine, can arise up to 18 days after vaccination, as seen in slide 16 of this CDC presentation. Both of these conditions typically require medical care.
Also, putting aside that CDC designed v-safe to capture medical care events beyond 7 days, our federal health agencies, highly reluctant to state negative things about a vaccine, also directly admit injuries can occur from vaccination more than 7 days after receiving the vaccine. Here are some examples:
HHS’s Vaccine Injury Table (hrsa.gov) (encephalopathy w/n 5-15 days, chronic arthritis w/n 7-42 days, thrombocytopenia w/n 7-30 days, GBS w/n 3-42 days);
FDA’s Peter Marks, MD, PhD, discusses COVID-19 vaccine at American ... (Dr. Marks, Director of FDA’s CBER, said in reference to Covid vaccine, though query how he could say this about a novel product, “We also asked for a minimum median of two months follow up … because most adverse events with vaccines appear within the first 42 days after vaccination.”);
Code of Federal Regulations (govinfo.gov) (For pandemic influenza vaccine, GBS w/n 3-42 days, PTS w/n 2-42 days).
To further point out the arbitrary nature of picking one week as the time frame to study, there are potentially concerning trends in seeking medical care within the v-safe dataset that occur after the first week of vaccination. For example, within seven days of dose 1 of a Pfizer vaccine, among those 3 years of age and older, .32% reported seeking medical care. But then look at the percentage of users seeking care in each succeeding interval, noting these figures are not cumulative:

I am not making any claims regarding what this chart means or could mean. I am merely pointing out that stopping at one week on this chart is arbitrary. Stopping at 42 days is also arbitrary. What doesn’t appear arbitrary is the trend in the first 42 days, yet this trend, under a standard of only reviewing medical care sought within the first seven days, will be missed or ignored by the CDC.
CDC Deceives the American People
Medical products cause harm. It happens. But what CDC did here is worse than any harm from any medical product. It is even worse than simply not telling the public the true rate of seeking medical care in the v-safe database.
Instead, CDC chose to actively mislead the public by repeatedly only publishing studies that looked at data from the first week after each dose of the vaccine. CDC knew this was, at best, highly misleading. This is what is incredibly concerning.
It is one thing to make a mistake – to overlook something. But here, CDC seemingly made a conscious choice to mislead the public on a critical issue. If the check-the-box v-safe data was not clawed out of the CDC’s hands through federal lawsuits, we would not know it engaged in this grand deception on the American people.
The numerous studies at the core of CDC’s claim that Covid-19 vaccines are safe are all deceptive by including only health impact data reported to v-safe following the first week after each dose. Had CDC instead included all of the data it actually chose to collect, it would have shown a seriously concerning rate of Americans seeking medical care after Covid-19 vaccination. That would not align with CDC’s claim the vaccine is safe.
CDC would have been better to not publish the data at all. At least it then would have just been withholding data, not actively deceiving. Instead, CDC actively chose to cherry-pick data in order to claim the vaccine is safe when it knew that the only data point it really had from the check-the-box data to determine whether the vaccines are safe had a blaring red alarm screaming “unsafe.” It just chose to hide that from the public.
And I wish I could say that is the worst of CDC’s conduct. But it is not. In the next part, we will discuss that when Reuters contacted CDC about the rate of users having to seek medical care, it simply lied! In a back and forth with CDC, through Reuters, it was clear the CDC was lying. Until then!
V-Safe Studies
V-Safe Studies: Adverse Events Days 0-7 After Vaccine
Safety monitoring of COVID-19 vaccine among children and young adul... (January 5, 2021)
COVID-19 vaccine safety update Advisory Committee on Immunization P... (January 27, 2021)
First Month of COVID-19 Vaccine Safety Monitoring - United States, ... (February 26, 2021)
COVID-19 vaccine safety update: Advisory Committee on Immunization ... (March 1, 2021)
Safety Monitoring of the Janssen (Johnson & Johnson) COVID-19 V... (May 7, 2021)
Reactogenicity Following Receipt of mRNA-Based COVID-19 Vaccines (June 1, 2021)
COVID-19 Vaccine safety updates: Advisory Committee on Immunization... (June 23, 2021)
COVID-19 Vaccine Safety in Adolescents Aged 12-17 Years - United St... (August 6, 2021)
Safety Monitoring of an Additional Dose of COVID-19 Vaccine - Unite... (October 1, 2021)
Early safety monitoring for additional COVID-19 vaccine doses: Repo... (October 21, 2021)
COVID-19 Vaccine Safety in Children Ages 5-11 years - United States... (December 31, 2021)
Safety Monitoring of COVID-19 Vaccine Booster Doses Among Adults - ... (February 18, 2022)
Safety Monitoring of COVID-19 Vaccine Booster Doses Among Persons A... (March 4, 2022)
Safety of mRNA vaccines administered during the initial 6 months of... (March 7, 2022)
Safety update of 1st booster mRNA COVID-19 vaccination Advisory Com... (April 20, 2022)
COVID-19 vaccine safety updates: Primary series in children ages 5–... (May 19, 2022)
Safety Monitoring of COVID-19 mRNA Vaccine First Booster Doses Amon... (July 15, 2022)
Reactogenicity of Simultaneous COVID-19 mRNA Booster and Influenza ... (July 15, 2022)
Safety Monitoring of COVID-19 mRNA Vaccine Second Booster Doses Amo... (July 29, 2022)
Safety Monitoring of Pfizer-BioNTech COVID-19 Vaccine Booster Doses... (August 19, 2022)
COVID-19 vaccine safety update: Primary series in young children an... (September 1, 2022)
Association between history of SARS-CoV-2 infection and severe syst... (November 1, 2022)
Safety of COVID-19 Vaccination in United States Children Ages 5 to ... (November 29, 2022)
Reactogenicity of Simultaneous COVID-19 mRNA Booster and Influenza ... (July 15, 2022)
Safety Monitoring of Bivalent COVID-19 mRNA Vaccine Booster Doses A... (November 4, 2022)
Safety Monitoring of Bivalent COVID-19 mRNA Vaccine Booster Doses A... (January 13, 2023)
V-Safe Studies: Adverse Events Days 0-7 After Vaccine & Free-Text to Day 14
Reactogenicity within 2 weeks after mRNA COVID-19 vaccines: Finding... (October 16, 2021)
V-Safe Studies: Free-Text Response Regarding Menstrual Irregularities
V-Safe Studies: Pregnancy and Birth Related Vaccine Impacts
Preliminary Findings of mRNA Covid-19 Vaccine Safety in Pregnant Pe... (April 21, 2021)
Receipt of mRNA COVID-19 vaccines preconception and during pregnanc... (August 9, 2021)
CDC v-safe COVID-19 Pregnancy Registry Team. Receipt of mRNA COVID-... (September 8, 2021)
COVID-19 vaccine safety in pregnancy : updates from the v-safe COVI... (September 22, 2021)
-
-
- The Cochrane Library recently updated its 2020 systematic review of physical interventions to reduce respiratory illnesses. The update included an additional 11 randomized controlled trials, bringing the total number of RCTs included to 78
- As in its 2020 review, they found no evidence to support the use of surgical face masks or N95 respirators to prevent influenza or COVID-19 infection
- The relative risk reduction of using surgical masks in the general population (within hospitals and communities at large) to reduce symptoms of flu-like/COVID-like illness (not lab confirmed) was a statistically insignificant 0.95
- The same goes for reducing laboratory-confirmed influenza and COVID. Here, the relative risk reduction was 1.01 with a confidence interval of 0.72 to 1.42. In other words, it’s a wash. On average, it raises your risk of lab-confirmed infection by 1%. Range-wise, it may lower your risk by 28% or raise it by as much as 42%
- The review also found “no clear differences between the use of medical/surgical masks compared with N95/P2 respirators”
The question of whether we should wear face masks or not to prevent the spread of COVID-19 has been a hotly contested issue ever since our so-called health authorities came out with the recommendation in early 2020. Some of us were quick to point out the obvious, namely that masks cannot filter out viruses due to the virus being far smaller than the holes in the fabric.
Surgical masks have only ever been used to prevent droplets of saliva to drip into open wounds during surgery, potentially causing an infection. That's all they were ever designed to do.
Numerous studies looking at mask-wearing during cold and flu season in years past came up empty, showing masks are not a viable prevention method. Yet the narrative we were fed was that masks will somehow prevent respiratory infection, and not wearing one meant you had no regard for the health and safety of others.
Never mind the fact that a healthy person cannot transmit disease in the first place. The asymptomatic spread fallacy was still used to reinforce the idea that everyone had to wear a mask, regardless of whether they were ill or not. You couldn't even debate the issue. The propaganda angle was the only viewpoint allowed to circulate.
Today, three years later, mask policies are cropping up yet again, especially in schools,1 and health care facilities. In December 2022, the Occupational Safety and Health Administration (OSHA) submitted a final rule to the Office of Information and Regulatory Affairs and Office of Management and Budget for review which, if approved and implemented, would make universal masking in health care facilities a PERMANENT rule.
The largest nursing union in the U.S., National Nurses United, is also pushing to include permanent rules for “screening and testing of patients, visitors and staff, measures ensuring optimal PPE, exposure notifications for healthcare workers and paid leave for those exposed or infected with COVID-19,” according to Health Care Dive.2 All of this despite the fact that the scientific underpinnings are now even shakier than they were in 2020.
The AARP (formerly the American Association of Retired Persons) is even going so far as to claim mask wearing can help prevent heart attacks!3 Florida Surgeon General Dr. Joseph Ladapo had the following to say about the AARP's attempt to invent benefits for mask wearers:4

Gold-Standard Scientific Review Published
The latest of these studies is a meta-analysis and systematic review by the Cochrane Library,5,6,7,8,9 an independent research organization that has been reviewing the use of physical interventions to reduce respiratory illnesses since 2010.10
Cochrane reviews have long been recognized as the gold standard in evidence-based health care as their analyses look at the whole body of published science, and every few years, reviews are updated to include the latest research findings.
For example, reports on "Physical Interventions to Interrupt or Reduce the Spread of Respiratory Viruses" were published in 2010, 2011, 2020 and January 30, 2023.
In the video above, Dr. Vinay Prasad, a hematologist-oncologist, health researcher and professor of epidemiology and biostatistics at the University of California, reviews11 the latest Cochrane review, which added 11 new randomized controlled trials (RTCs) and cluster-RCTs to their previous 2020 analysis.
That brings the total number of RCTs included in the systematic review to 78. Six of the 11 new RCTs were conducted during the COVID pandemic and looked at the spread of COVID-19 specifically.
Still No Evidence to Back Surgical Mask Recommendations
The Cochrane investigators concluded that, while there's "uncertainty about the effects of face masks" due to trial bias and low adherence by participants, the pooled results of randomized controlled trials (RTCs) "did not show a clear reduction in respiratory viral infection with the use of medical/surgical masks." Here's an excerpt from the review:12
"Medical or surgical masks — Ten studies took place in the community, and two studies in healthcare workers.
Compared with wearing no mask in the community studies only, wearing a mask may make little to no difference in how many people caught a flu‐like illness/COVID‐like illness (9 studies; 276,917 people); and probably makes little or no difference in how many people have flu/COVID confirmed by a laboratory test (6 studies; 13,919 people)."
The relative risk reduction of using surgical masks in the general population (within hospitals and communities at large) to reduce symptoms of flu-like/COVID-like illness (not lab confirmed) was 0.95.
A value below 1 indicates the intervention improved outcomes, whereas a value above 1 shows it made it worse. So, here, surgical masks was associated with a relative risk reduction of 5%.
However, it's not statistically significant, as the confidence interval ranges from 0.84 to 1.09.13 So, it may lower your risk by as much as 16% or raise it by 9%. As noted by Prasad, the most accurate way to describe this finding is that "we have not proven there is an effect."
This is conclusive … This is the reality … You just don't have credible evidence [for masking], and the science didn't change … This is what the science has always shown. ~ Dr. Vinay Prasad
The same goes for reducing laboratory-confirmed influenza and COVID. Here, the relative risk reduction was 1.01 with a confidence interval of 0.72 to 1.42. In other words, it's a complete wash. On average, it raises your risk of lab-confirmed infection by 1%. Range-wise, it may lower your risk by 28% or raise it by as much as 42%.
So, masking really has no effect on confirmed infection rates (which, by the way, is more important than reports of perceived symptoms). As noted by the authors, the analysis "suggests that wearing a medical/surgical mask probably makes little or no difference compared to not wearing a mask for this outcome."
"This is conclusive," Prasad says. "This is the reality … You just don't have credible evidence [for masking], and I want to tell you this: The science didn't change … This is what the science has always shown."
Download this Article Before it Disappears
Download PDFN95 Masks Are Useless Too
The review also found "no clear differences between the use of medical/surgical masks compared with N95/P2 respirators." As detailed by the authors:14
"N95/P2 respirators — Four studies were in healthcare workers, and one small study was in the community. Compared with wearing medical or surgical masks, wearing N95/P2 respirators probably makes little to no difference in how many people have confirmed flu (5 studies; 8407 people); and may make little to no difference in how many people catch a flu‐like illness (5 studies; 8407 people), or respiratory illness (3 studies; 7799 people)."
Public Health Experts Simply Lied
So, in conclusion, none of the new studies that were added made one iota of difference. Masks were unable to prevent influenza transmission before the pandemic, and they still fail to prevent respiratory infections, be it the flu or COVID.
But, if there was no evidence to back masking in the first place, how did we end up with mask mandates? In short, our public health authorities started lying. As noted by Prasad: "Anthony Fauci told the truth on '60 Minutes' — the first time. The second time when he said you have to wear a cloth mask … he was lying."
Yet somehow, they managed to convince everyone that the truth was the lie and the lie was the truth.
A clip from Fauci's "60 Minutes" appearance is featured in "The Jimmy Dore Show" video above, as are some of his later public announcements where he suddenly promotes mask wearing and defends mask mandates.
Population-Wide Mask Mandates 'Never Made Sense'
In a February 3, 2023, article in The Spectator,15 lead author Tom Jefferson and Carl Heneghan, director of the University of Oxford's Centre for Evidence-Based Medicine and former editor-in-chief of BMJ Evidence-Based Medicine, explained why the 2020 Cochrane review was unable to influence public health policy on masking:
"This is the second update of the review since the start of the pandemic. The first update was delayed by seven months due to unexplained editorial decisions. It was too late when it came out in November 2020 to make a difference to national COVID policy; by then, activism, low-quality observational evidence and government policy had set the agenda for mask mandates, and the damage had been done.
Often these government policies relied on observational studies on mask usage and the spread of COVID. But there are lots of flaws in observational evidence.
For example, in the absence of a study protocol setting out methods before the study is done, it is possible to shift the dates of an observational analysis to suit the rise and fall in infections. So if you time your analysis near the peak of infections, the results will favor mask interventions as the infection rate quickly decreases.
But when we pointed out in November 202016 the troubling lack of robust evidence on face masks and the problems with observational studies, we were shouted down, removed from Facebook and put on the government's secret watchlist …
Mandates that affected the whole population never made sense … even in high adherence populations such as Japan, they have not stemmed an inevitable rise in infections. Part of the problem may be that during the pandemic the government had to be seen to be doing something. Interventions like handwashing and vaccines are invisible, but masks acted as a visible sign of compliance.
What we have witnessed in this pandemic are strong beliefs about what works and what doesn't … Several policies such as mask mandates, restrictions, and unproven interventions now seem absurd in hindsight. And as the culture of fear has lifted, the population has become all too aware of their detrimental effects.
We failed to follow an evidence-based approach during the pandemic. We are now left with the human, social and economic aftermath of evidence-free policies."
Public Health Agencies 'Steeped in Failure'
As noted by Prasad in an accompanying Substack post:17
"Who should we be angry with? Obviously there is a class of twitter expert that doesn't understand how to read evidence. Some of them have even been promoted to be deans for public health schools. So much for public health.
But the real failure is NIAID [National Institutes of Allergy and Infectious Diseases] and CDC [U.S. Centers for Disease Control and Prevention]. It is Tony Fauci.
Fauci controlled NIAID budget. He could have run 10 RCTs of masking — different masks, different ages, different settings. He chose to run zero. Instead he went on TV 1,000 times and lied about effectiveness of cloth masks …
CDC and AAP [American Academy of Pediatrics] are also steeped in failure. These agency forced 2 year olds to mask. Against the advice of the World Health Organization and UNICEF.
The Cochrane review fails to identify any data that pertains to 2 year olds. The CDC should be ashamed of themselves. Tens of thousands of people working from home, and no one inside the organization with the ability to stop this policy."
Scientists Censored by Propagandists
Perhaps the most disturbing aspect of this masking debacle has been the massive censorship and shutting down of healthy scientific debate, not just among laypeople but among scientists themselves.
Only the yes-men were ever given room to air their perfectly scripted views, while those who had concerns were silenced, regardless of their credentials. YouTube even censored a roundtable discussion with Florida Gov. Ron DeSantis and several medical experts. Why? Because in multiple instances, the doctors said children didn't need to wear masks, and this position violated YouTube's "COVID-19 medical misinformation" policy.
In a February 6 Substack article, Jefferson describes the propaganda effort to twist the findings of the 2023 Cochrane review on masking and other physical interventions against COVID-19:18
"We, the co-authors of the Cochrane review … have received several … 'can I please check the main facts and, by the way, tell me what your review says because I cannot be bothered to do my job' type of messages. However, we recently got another query … This request comes from a very powerful press syndicate:
'I'm reaching out because I've been seeing some posts [links redacted by TJ] spreading widely on social media that seem to be misrepresenting the conclusions of your recently published study on physical interventions and respiratory viruses.
Do you think it is a misrepresentation to claim (as the tweets I link to above do) that your study definitively proves that masks don't work in preventing the spread of viruses such as COVID-19 and the flu? If so, I'd be interested in debunking these claims to set the record straight and would love to speak with you more about the study.'
The disturbing aspect of this request is as follows: the stringer is making contact with one of us. After exchanging pleasantries, he/she will ask a few superfluous questions.
We have an abstract, a plain language summary, TTE [Trust the Evidence] posts and a podcast, and Carl and I have written a Spectator piece covering the review. If you are a real masochist, you can read all the 300-plus pages of the review …
So there is nothing to explain or fact-check. But the stringer is not really interested in checking facts. What they want to do is to write truthfully that they have spoken to one of us and then put the spin required in the release to ensure the 'misinterpretation' of twitterati is set straight. 'Debunking' is the term used, and it will be actioned if the stringer thinks the Twitterati have 'misinterpreted' our findings …
What disturbs me … is the idea of 'debunking' or 'normalization' of the information flow. We have done the tough work over two decades, reporting results separately from our interpretation, as in all Cochrane reviews. The studies' results are the results reported by the authors of the single studies included in the reviews.
Our interpretation is one you can — and should if you want — challenge. However, successfully challenging our interpretation requires hard work, elbow grease, graft, focus, and application. So picking up the phone and speaking to someone, then deciding how to 'debunk' or normalize the message, is so much easier.
The reach of this particular press syndicate is global and powerful. I wonder why the stringer wanted to 'debunk' the interpretation of the twitterati mentioned in the text. To ensure 'truth' triumphed? Or to ensure no more waves in the official narratives were made by a bunch of academics or Twitter dwellers?"
While Jefferson now avoids interactions with the mainstream media, he did agree to an interview with investigative journalist Maryanne Demasi, which you can read here.19 He also granted an interview with Paul D. Thacker, which you can read on Thacker's Substack.
Pro-Maskers Guilty of Creating Massive Pollution Problem
In addition to the many health problems associated with prolonged mask wearing, which I've addressed previously, mask policies have also created a massive pollution problem. Ironically, many pro-mask activists also claim to be environmentalists, yet they completely ignore the environmental effects of mask mandates.
According to UNICEF, the world used and discarded an estimated 2.4 billion masks in 2020.20 Another estimate, calculated by the University of Southern Denmark,21 put that number at 129 billion face masks EACH MONTH. As reported by Business Insider:22
"Since the very first lockdowns of 2020, these plastic-based coverings have … been an environmental disaster in the making … [The] rapid adoption of face masks … means their waste can now be found everywhere …
Discarded masks have seeped into every corner of our lives, from city sidewalks to solemn niches of the internet.23 They've washed up on the shores of Hong Kong's deserted Soko Islands and cloaked octopi off the coast of France.
Scientists and environmental advocates expressed alarm24 about this tsunami of waste … They foresaw the dire ecological ramifications of our mask waste — especially once those masks made their inevitable way into the earth's waterways.
Elastic loops pose entanglement hazards for turtles, birds, and other animals. Fish could eat the plastic-fiber ribbons that unfurl from a discarded mask's body. Then, there is the untold menace to human health that would likely present, at the microscopic level, once masks began to disintegrate."
The global consumption of other single-use plastics also increased by a whopping 300% in the last three years, further adding to the problem of plastic pollution. You'd think governments that claim to be so concerned about "saving the planet" would address the issue, but no. As noted by Business Insider:25
"[W]orld leaders have ignored the problem. And once the immediate public-health emergency superseded ecological concerns — the heads of Big Plastic made sure it stayed that way."
Medical Masks Are Hazardous Waste
Research26 from Swansea University in Wales reveals single-use masks readily disintegrate when submerged in water, releasing both micro- and nanoplastic particles, even after relatively brief periods of submersion.27
As if that's not bad enough, the masks also release nanoparticles of heavy metals like lead, cadmium, copper and arsenic. Not only can this mask litter result in contaminated drinking water, but the particles can also disrupt entire marine food chains.
Nanoparticles are particularly troublesome as they can penetrate cell walls and damage DNA, and this is true not just in animals and humans but also in plants. As reported by Business Insider:28
"Recent research29 on silicon nanoparticles, in particular, has shown that if a particle is very small in nano scale, it can act almost as a tiny, carcinogenic bomb. Multiply that by a minimum of several hundred per mask, at a rate of 50,000 masks disposed per second, and the scope of the dilemma grows vivid."
According to research30 published in Science of the Total Environment in September 2021, the polypropylene in medical face masks could be recycled either by mechanical or thermal means, and biodegradable mask options are also available. Yet no one in a position of power is advocating for these solutions.
High Time to Discard False Mask Narratives
It's time to put an end to the false narratives that mask wearing lowers infection rates and/or that it "protects others." They protect no one. Not the wearer and not those around the wearer.
And, as noted by Prasad in the featured video, the burden of proof lays on the proponent of a given intervention. In this case, those claiming we should mask up to protect others are the ones who have the responsibility to prove they're correct. The burden of proof is not on those who object, based on logical and existing evidence.
Universal mask wearing is also resulting in environmental pollution that is completely unnecessary and avoidable. So, please, just stop wearing disposable masks. It's time. The record has been set straight. There are no benefits, and plenty of risks and negative impacts.
-
-

-
-
Are Enzymes a Key to COVID Endothelial Injury?
Analysis by Dr. Joseph MercolaFact Checked
- February 10, 2023
STORY AT-A-GLANCE
- Studies suggest damage to the endothelium, which are cells covering blood vessels, is contributing to the development of blood clots, or thrombosis, in the blood vessels of severely ill COVID-19 patients
- Enzymes may turn out to be the missing link in helping to break up clusters of clotting proteins involved in this dangerous thrombosis, which is linked to increased mortality in COVID-19
- Levels of Von Willebrand factor (VWF), a clotting protein released by endothelial cells, were found to be significantly elevated in COVID-19 patients in advanced stages of the disease
- Proteolytic enzymes such as lumbrokinase, serrapeptase and nattokinase also act as natural anticoagulants by breaking down the fibrin that forms blood clots
From Dr. Joseph Mercola
Since COVID-19 first entered the scene, exchange of ideas has basically been outlawed. By sharing my views and those from various experts throughout the pandemic on COVID treatments and the experimental COVID jabs, I became a main target of the White House, the political establishment and the global cabal.
Propaganda and pervasive censorship have been deployed to seize control over every part of your life, including your health, finances and food supply. The major media are key players and have been instrumental in creating and fueling fear.
I am republishing this article in its original form so that you can see how the progression unfolded.
Originally published: November 30, 2020
Enzymes catalyze many biological reactions in your body. They regulate the rate of these chemical reactions, speeding them up so necessary functions like digestion, muscle contractions and other aspects of cellular metabolism can occur.1
Enzymes are also emerging as key players in COVID-19, as studies suggest damage to the endothelium, which are cells covering blood vessels, is contributing to the development of blood clots, or thrombosis, in the blood vessels of severely ill COVID-19 patients.2 Enzymes may turn out to be the missing link in helping to break up clusters of clotting proteins involved in this dangerous thrombosis.
Endothelium Damage Found in Critically Ill COVID-19 Cases
After noticing blackened fingers and toes — signs of what appeared to be microvascular thrombosis, or tiny blood clots in small blood vessels — in COVID-19 patients in advanced stages of the disease, physicians at the Yale School of Medicine began running clotting tests on their patients.3
Levels of Von Willebrand factor (VWF), a clotting protein released by endothelial cells, were found to be significantly elevated, which suggested to hematologist Alfred Lee that damaged endothelial cells may be releasing large quantities of VWF, leading to clots.4 This prompted the team to screen for additional markers of endothelial cell and platelet activation in critically and noncritically ill COVID-19 patients.
The study, which was conducted in April 2020, included 68 hospitalized patients with COVID-19 and 13 asymptomatic controls. VWF antigen was significantly elevated in COVID-19 patients admitted to the intensive care unit (ICU) compared to non-ICU COVID-19 patients,5 as was soluble platelet selectin (sP-selectin), which is sometimes used as a biomarker for infection and mortality.6
Specifically, mean VWF was 565% among ICU patients and 278% among non-ICU patients while soluble P-selectin was 15.9 ng/mL compared to 11.2 ng/mL.7 "Our findings show that endotheliopathy is present in COVID-19 and is likely to be associated with critical illness and death. Early identification of endotheliopathy and strategies to mitigate its progression might improve outcomes in COVID-19," the researchers concluded.8
Likely not coincidentally, endothelial dysfunction is also associated with insulin resistance and plays a role in the vascular complications of diabetes,9 as well as being involved in obesity and high blood pressure,10 conditions that raise the risk of severe COVID-19.
Even mild obesity may raise the risk of COVID-19 severity — COVID-19 patients with mild obesity had a 2.5 times greater risk of respiratory failure and a five times greater risk of being admitted to an ICU compared to nonobese patients. Those with a BMI of 35 and over were also 12 times more likely to die from COVID-19.11
Another study looking into the impact of coexisting health conditions like high blood pressure, heart disease and diabetes on COVID-19 outcomes found they're linked to "poorer clinical outcomes," such as admission to an intensive care unit, a need for invasive ventilation or death.12
It's possible that the endothelial damage in all of these conditions plays a role in worsening COVID-19 outcomes, but it's unclear which comes first — endothelial damage or COVID-19.
Endothelial Cells Are the 'Main Target' of SARS-CoV-2
Imperial College London cardiologist Thomas Lüscher told The Scientist that the endothelium is the main target of SARS-CoV-2, the virus that causes COVID-19.13 Under healthy conditions, blood cells can pass through the endothelium lining blood vessels, but when exposed to viral infections and other inflammatory agents, the endothelium becomes sticky and releases VWF.
The end result is a cascade of clotting and inflammation, both characteristics of severe COVID-19. According to a case report published April 8, 2020, "A hallmark of severe COVID-19 is coagulopathy, with 71.4% of patients who die of COVID-19 meeting … criteria for disseminated intravascular coagulation (DIC) while only 0.6% of patients who survive meet these criteria."14
Writing in the European Heart Journal, Lüscher argues, "COVID-19, particularly in the later complicated stages, represents an endothelial disease,"15 which may help explain why multiple organ systems, including the lungs, heart, brain, kidney and vasculature, may be affected.
An additional study by Canadian researchers, published in Critical Care Explorations in September 2020, also revealed elevated VWF and soluble P-selectin levels in COVID-19 patients, along with higher glycocalyx-degradation products,16 a sign of damage to the glycocalyx, which envelops the endothelium.17 This can also be a sign of sepsis. Taken together, the research suggests that therapies targeting the endothelium may be useful for COVID-19, which is where enzymes come in.
Download this Article Before it Disappears
Download PDFEnzymes Used to Treat COVID-19
With the role of coagulopathy in severe COVID-19 becoming clearer, researchers have experimented with enzymes in the treatment of the disease. Fibrinolytic therapy, which uses drugs or enzymes to break up blood clots, has been used in a Phase 1 clinical trial that showed the treatment reduced mortality and led to improvements in oxygenation.18 Further, researchers wrote in the Journal of Thrombosis and Haemostasis:19
"There is evidence in both animals and humans that fibrinolytic therapy in acute lung injury and acute respiratory distress syndrome (ARDS) improves survival, which also points to fibrin deposition in the pulmonary microvasculature as a contributory cause of ARDS.
This would be expected to be seen in patients with ARDS and concomitant diagnoses of DIC on their laboratory values such as what is observed in more than 70% of those who die of COVID‐19."
The researchers reported three case studies of patients with severe COVID‐19 respiratory failure who were treated with tissue plasminogen activator (TPA), a serine protease enzyme found on endothelial cells that's involved in fibrinolysis, or the breakdown of blood clots.20
All three patients benefited from the treatment, with partial pressure of oxygen/FiO2 (P/F) ratios, a measure of lung function, improving from 38% to 100%.21 While it should be noted that several of the authors have patents pending related to both coagulation/fibrinolysis diagnostics and therapeutics, the results suggest such treatments deserve further evaluation in certain COVID-19 patients.
An evaluation of organ tissues from people who died from COVID-19 also revealed extensive lung damage, including clotting, and long-term persistence of virus cells in pneumocytes and endothelial cells.22
The findings indicate that virus-infected cells may persist for long periods inside the lungs, contributing to scar tissue. In an interview with Reuters, study co-author Mauro Giacca, a professor at King's College London, described "really vast destruction of the architecture of the lungs," with healthy tissue "almost completely substituted by scar tissue,"23 which could be responsible for cases of "long COVID," in which symptoms persist for months.
"It could very well be envisaged that one of the reasons why there are cases of long COVID is because there is vast destruction of lung (tissue)," he told Reuters. "Even if someone recovers from COVID, the damage that is done could be massive."24 Dissolving scar tissue is another area where enzymes, particularly proteolytic enzymes, may be useful.
Three Top Enzymes Act as Natural Anticoagulants
Holistic prophylactic alternatives that might be beneficial against blood clots include proteolytic enzymes such as lumbrokinase, serrapeptase and nattokinase, all of which act as natural anticoagulants by breaking down the fibrin that forms the blood clot. Fibrin is a clotting material that restricts blood flow, found both in your bloodstream and connective tissue such as your muscles. Fibrin accumulation is also responsible for scar tissue.
It is important to understand that when using these enzymes for fibrinolytic therapy they need to be taken on an empty stomach, at least one hour before or two hours after meals. Otherwise these enzymes will be wasted in the digestion of your food and will be unable to serve their fibrinolytic purpose.
As noted in Scientific Reports, some of the key mechanisms by which proteolytic enzymes exert their anticoagulant effect include "defibrinogenation, inhibition of platelet aggregation, and/or interference with components of the blood coagulation cascade."25 Here's a closer look at these important enzymes, all of which are available in supplement form or, in the case of nattokinase, via the food natto.
1.Lumbrokinase — This enzyme is about 300 times stronger than serrapeptase and nearly 30 times stronger than nattokinase,26 making it my strong personal preference and recommendation if you are using a fibrinolytic enzyme. Extracted from earthworms, lumbrokinase is a highly effective antithrombotic agent that reduces blood viscosity and platelet aggregation27 while also degrading fibrin, which is a key factor in clot formation.
2.Serrapeptase — Also known as serratiopeptidase, serrapeptase is produced in the gut of newborn Bombyx mori silkworms, allowing them to dissolve and escape from their cocoons. Research has shown it can help patients with chronic airway disease, lessening viscosity of sputum and reducing coughing.28 Serrapeptase also breaks down fibrin and helps dissolve dead or damaged tissue without harming healthy tissue.29
3.Nattokinase — Produced by the bacteria Bacillus subtilis during the fermentation of soybeans to produce natto,30 nattokinase is a strong thrombolytic31 comparable to aspirin but without the serious side effects.32
It's been shown to break down blood clots and reduce the risk of serious clotting33 by dissolving excess fibrin in your blood vessels,34 improving circulation and decreasing blood viscosity. Interestingly, in one in vitro study, the thrombolytic activity of equivalent amounts of nattokinase and TPA were found to be identical35 — TPA, remember, is the enzyme that led to improvement in the three COVID-19 case studies.36
-
-
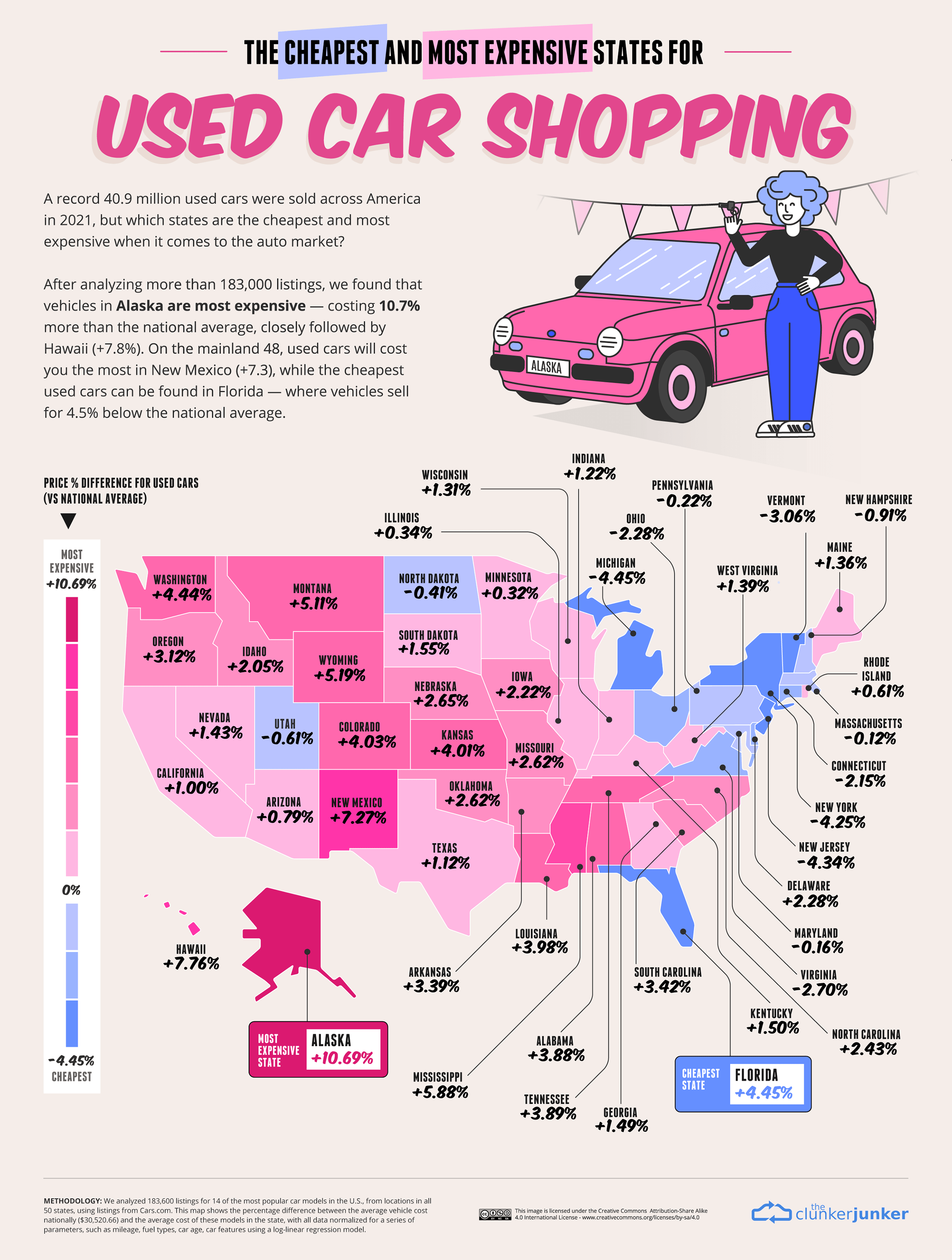
About
© 2025 Created by carol ann parisi.
Powered by
![]()