The Great Awakening-In God We Trust
FROM MERCOLA C-19 Injections: Massive Regulatory and Manufacturing Fraud
C-19 Injections: Massive Regulatory and Manufacturing Fraud
Analysis by Tessa LenaC-19 Injections, Regulatory and Manufacturing Fraud: Tessa Lena Tal...
C-19 Injections, Regulatory and Manufacturing Fraud: Tessa Lena Tal...
C-19 Injections, Regulatory and Manufacturing Fraud: Tessa Lena Tal...
C-19 Injections, Regulatory and Manufacturing Fraud: Tessa Lena Tal...
- Alexandra Latypova is an ex-pharmaceutical industry and biotech executive with a lot of experience in the areas of drug safety and clinical trials
- Early on, she discovered that, based on the number of reported deaths and adverse events per lot, there was unprecedented variability in the toxicity of the product
- According to Alexandra, the mRNA shots do not conform to their label specifications, and “in practice, both ‘blank’ and ‘lethal’ vials and anything in between is produced”
- Having analyzed massive amounts of publicly available data, as well as documents that became available as a result of FOIA requests and other sources, she has found strong evidence of manufacturing and regulatory fraud
I recently had the pleasure of interviewing Alexandra Latypova, an ex-pharmaceutical industry and biotech executive, who has been investigating and exposing manufacturing and regulatory fraud related to COVID injections.
We talked about the industry standards that were not adhered to during the clinical trials and the manufacturing of those injections, about the vial content quality testing procedures that had not been put in place, about the "hot batches" and their geographical distribution, about signs of fraud at every stage of testing and manufacturing the product, and about the general condition of living in a world run by a mob.
The latter was the lightest part of our conversation — evoking a lot of dark Eastern European humor — since both of us are Soviet expats, and in 2020, neither of us required a whole lot of imagination to embrace the existential possibility of living in a world run by a mob. We had seen it in the past without a disguise — and when something looks like a duck, walks like a duck, and quacks like a duck, maybe it's just a duck!
Alexandra Latypova's Background
Alexandra grew up in Soviet Ukraine and immigrated to America in the late 1990s. She received her MBA from Dartmouth College and the spent about twenty five years in pharmaceutical industry and biotech (including in the areas of drug safety and clinical trials).
Alexandra has had a very gratifying entrepreneurial career. She has founded a number of successful startups, sold them — all before COVID — and retired, hoping to focus on enjoying her life and especially painting, which she does masterfully.
When 2020 knocked on the door with a whole bag of ugly and weird "new normal" treats, Sasha smelled the rat right away. Initially, she became alarmed by the abnormalities in "COVID response," including the very conspicuous campaign to prevent effective treatment of COVID.
Compelled to understand what was going on, Alexandra got to work. She looked at VAERS and discovered huge discrepancies between the lots, where some batches had just a few reported severe adverse events, and some had over 1500 (she later learned from FOIA'ed documents that lot sizes were in a relatively similar range, and thus the discrepancies could not be explained by the lot size).
And when it comes to VAERS, let's not forget the 2010 Harvard Pilgrim study showing that VAERS was severely underreported — NOT overreported — capturing less than 1% of adverse events.
"Hot Batches"
Early on, Alexandra discovered the existence of "hot batches." She is one of team members behind the famous "How Bad Is My Batch" webpage where people can look up the number of severe adverse events reported to VAERS associated with a COVID injection lot number. Other fearless members of the team are Dr Mike Yeadon, ex-head of Pfizer Respiratory Research, Jessica Rose, statistician, Craig Paardekooper, researcher, and Walter Wagner, lawyer.
The slide below show the unprecedented variability of serious adverse events and deaths in the U.S. per batch. Note the comparison to the variability of the flu vaccine lots.
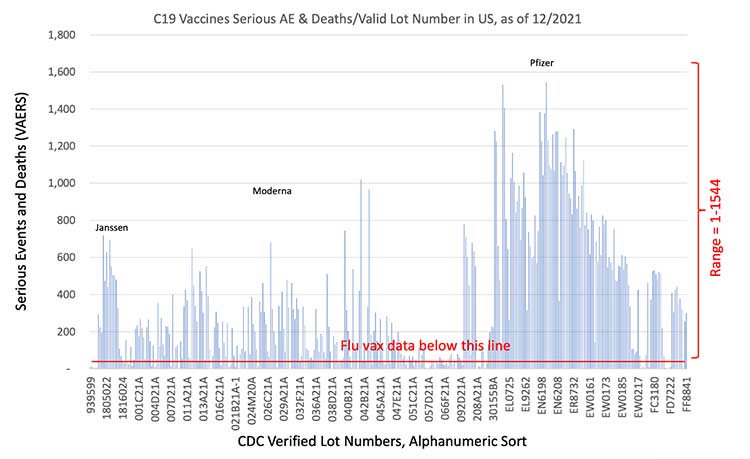
In the interview, Alexandra also mentioned the uneven distribution of deaths per a hundred thousand doses from batch to batch in the U.S. The coasts did much better than some of the Midwestern states that showed a very high numbers of reported deaths per a hundred thousand doses. The worst state is South Dakota (30+ reported deaths per 100,000 doses).
The areas that did even worse, according to Alexandra, were some of the U.S. territories with high percentage of indigenous population. (The latter data became available after the presentation was created, not reflected in the slide.)

"Garbage Soup": Non-Compliance With Good Manufacturing Practices
In the interview, Alexandra calls the COVID injections products "garbage soup," both due to the massive non-compliance of the vial content to the specifications (per multiple independently done tests) — as well as due to their non-compliance with Good Manufacturing Practices. Wait, are the manufacturers trolling us? Are telling us that they do not comply (but we must)?!
There are many theories about what's behind for such wild inconsistency between batches, from manufacturing defects to deliberate toxicity testing — and anything in-between. In her TrialSiteNews article, Alexandra tackles one important angle of the challenge that so many of us had to "explain" when talking to the friends of a more mainstream persuasion:
"Many of us are familiar with the following conundrum: on one hand, highly credentialed scientists and doctors have written numerous research papers explaining the dangerous mechanisms of action underlying mRNA/DNA "platform" technologies. The papers are meticulously researched and depict, correctly in my opinion, many terrifying consequences of the technology that breaches the innate protective mechanisms of human cells."
"Furthermore, these theoretical papers are validated by the observed outcomes, such as for example, increases in all-cause mortality in high correlation with increases in rates of vaccination in a given territory, unprecedented increases in the adverse events and deaths recorded by various passive reporting systems, astonishingly high reports of the adverse events and deaths from the pharmas' own pharmacovigilance systems, and autopsy findings in vaccinated post-mortem showing the mechanisms of mRNA technology damage in histopathologic evaluations.
On the other hand, many who have received the injections report no adverse effects and deem the points above a 'crazy conspiracy.'"
"The question from the uninjured seems to be – why don't we see MORE deaths if what you say about mRNA products is true? Setting aside ethical limitations of this question, here is a possible answer why: The mRNA shots do not conform to their label specifications. In practice both "blank" and "lethal" vials and anything in between is produced [emphasis mine]."
Like I wrote earlier on my Substack, "remarkably, some analyzed vials were reported to contain left over magnetic beads (magnetic beads are used in production of mRNA). Remember the "crazy" videos of some people developing magnetism in the place of injection? Now we have a new, 'non-conspiratorial' explanation for the 'conspiratorial' videos! Yay, following the science!"
According to Alexandra, vials of mRNA injections are not routinely tested by the manufacturers for conformity to the label. She notes that "the more they conform to the mRNA specification, the deadlier they seem."
The only vial-level tests specified, for instance, by Pfizer, in leaked Chemistry Manufacturing and Controls documents, are the vial weight at filling, manual inspection for large visible particles, and some tests related to integrity such as vial capping.
The documents don't describe no routing vial or dose tests verifying the ingredients. Each Pfizer dose is supposed to contain 30 mcg of mRNA, as stated on the label, but there is no information about any testing done to verify that.
"The ingredient conformity tests described in Pfizer CMC package are based on the bulk product batch testing – an upstream manufacturing process step.
It is a regulatory requirement to retain samples of each batch produced, and these samples of vials should exist and be available for examination. Per contracts with the US Government/DOD, the product is shipped to the DOD who retains the ownership of the vials until the product is injected into people."
Alexandra notes that those contracts are very detailed and specify manufacturing data to be delivered to the DOD, however, she not find any descriptions of sampling of the vials for purposes of verification of their contents vs the label. "Furthermore, it is expressly forbidden by the international vaccine supply contracts to perform the vial tests for label conformity."
Evidence of Collusion
In the interview, as well as in this article, Alexandra talks about the evidence of collusion between the manufacturers, the global regulatory agencies, and the US Department of Defense.
Having analyzed various public data from CDC's VAERS database as well as various documents that have been obtained through FOIA releases and other source, she concluded that such collusion "led to the commercial release of the Covid-19 countermeasures that do not comply with the current Good Manufacturing Practices (cGMP)."
Evidence that Alexandra talks about includes Moderna's non-clinical study summaries, Pfizer's Chemistry Manufacturing and Controls documentation, and contracts between pharma and the DOD for supply of the mRNA/DNA products. According to her, "it reveals disregard for established safety rules, regulations, and safety practices throughout the development, manufacture, and distribution of these products."
Moderna Red Flags
As reported by Children's Health Defense, Alexandra reviewed 700 pages of documents that Moderna submitted to the FDA as part of its application process and obtained via a Freedom of Information Act request.
And according to her, "out of nearly 700 pages, about 400 pages are irrelevant studies that Moderna repeated multiple times. Moderna also submitted three versions of a single module, she said. And one module contained only narrative summaries of Moderna's studies, but no actual study results." Alexandra's conclusion is that we are missing a large number of results, such as full reports that would support their narrative.
"The FDA 'obviously did not object' to any of this, she said. 'That's evidence of collusion to me with the manufacturer.'"
Other "abnormalities" that Alexandra highlighted both in the interview and in the Children's Health Defense article, were Moderna's clinical trials timeline and the fact that their product has two — not one — Investigational New Drug (IND) number.
Normally, there is one IND application for one product. "In this case, however, there are two IND applications — one belonging to Moderna, and one belonging to the National Institutes of Health, which partnered with Moderna on its COVID-19 vaccine."
"The Investigational New Drug (IND) application meeting is supposed to occur with the FDA when the company initiates human clinical trials. Moderna and the FDA had a pre-IND meeting on Feb. 19, 2020, and the IND application was formally opened the next day. The global pandemic was declared on March 11, 2020."
In the words of Alexandra, "Somehow these visionaries could predict the future with such certainty that they opened a clinical trial for the vaccine, for which a pandemic was announced a month later."
Pfizer Red Flags
As Alexandra notes in her article titled, "Did Pfizer Perform Adequate Safety Testing for its Covid-19 mRNA Vaccine in Preclinical Studies? Evidence of Scientific and Regulatory Fraud," "both the manufacturer and the regulators behaved in a highly dishonest manner and conspired to push an entirely novel technology and product on millions of people without carrying out a single well designed safety assessment."
For example, she points out that a review of clinical studies released by FOIA uncovered that at least 4 different variants of active ingredient were included in the single Investigational New Drug application by Pfizer IND#19736:
- BNT162a1 — Unmodified mRNA (uRNA; variant RBL063.3)
- BNT162b1 — Methylpseudouridine-modified mRNA (modRNA; variant RBP020.3)
- BNT162b2 — Methylpseudouridine-modified RNA (modRNA; variant RBP020.2)
- BNT162c2 — Self-amplifying unmodified mRNA (saRNA; variant RBS004.2)
Alexandra writes that while the use of multiple versions of a product in the early stages of development is often inevitable, each chemical or biological entity is nevertheless deemed legally distinct for the purpose of product approval.
"Therefore, studies conducted with versions of the product that don't conform to the exact specification of the final version may serve only as supporting information for the approval of the latter, but they should never be deemed definitive and sufficient tests for claims of safety or efficacy pertaining to the final product."
She further mentions that in September 2021, the FDA issued a draft guidance entitled "Studying Multiple Versions of a Cellular or Gene Therapy Product in an Early-Phase Clinical Trial," which states that each version of product requires a separate IND application.
However, stunningly, "a footnote in this guideline exempts 'vaccines intended to prevent infectious diseases' from this requirement. No explanation is given as to why this exemption is made, and no conceivable scientific or legal basis exists for this exemption, other than that the FDA had already arbitrarily allowed this unprecedented deviation from the regulatory standard and later needed to cover their tracks.
In fact, arguably this regulatory 'exception' does not even apply to Pfizer's COVID-19 'vaccine,' since the product does not prevent infection or transmission of the disease. Is intent to prevent illness alone a sufficient condition? After all, every new drug is intended to do something like preventing an illness, but only few successfully do so."
Alexandra's article is very detailed, and I highly recommend reading it in full. You can also find Alexandra on TrialSiteNews and on her Bitchute channel. To summarize her take on Pfizer, she make the following points:
•Pfizer's program did not include a comprehensive end-to-end test of all components of the final approved product (the mRNA COVID-19 vaccine). Instead, the studies included in the document package submitted to the FDA employed several variants and analogues of the product, whose comparability to the actual COVID-19 vaccine was not demonstrated or evaluated.
Thus, no comprehensive assessment of product safety can be made on the basis of these studies.
•A key determinant of a drug's toxicity is its distribution within the body. However, with the mRNA active ingredient of Pfizer's COVID-19 vaccine, this crucial aspect was never studied!
•Pfizer claimed absence of potential for "vaccine-elicited disease enhancement" based on studies of an animal species that does not get sick from SARS-CoV-2.
•The CDC, the FDA and Pfizer all lied about "vaccine staying at the injection site;" they knew all along that distribution of the vaccine throughout the body had to be expected.
•Pfizer skipped major categories of safety testing altogether.
•Pfizer used dishonest and self-serving interpretation of regulatory guidelines to justify the shortcuts it took in routine safety testing.
•Both FDA and Pfizer knew about major toxicities associated with gene-therapy medicines in general, and they therefore cannot claim lack of anticipatory knowledge of these risks with the particular gene therapy medicine that is Pfizer's COVID-19 vaccine. This points to intentional fraud and collusion between Pfizer and the regulators, who conspired to push this untested dangerous product on the market.
Views: 16
Comments are closed for this blog post
-
Comment by carol ann parisi on November 22, 2022 at 5:19pm
-
-
Pfizer’s Financial Supernova and the Art of Really Big Lies
Analysis by Dr. Joseph MercolaFact Checked
mRNA isn't leaving the body. It's everywhere! (bitchute.com)- November 22, 2022
STORY AT-A-GLANCE
- Pfizer’s annual revenue is expected to reach $101.3 billion in 2022, thanks to its COVID jab, which doesn’t prevent infection or spread, and Paxlovid, an ineffective and dangerous COVID antiviral that causes rebound
- Pfizer got plenty of free help from the federal government, which bullied and harassed people into getting the shots, and implemented rules that ensure hospitals and pharmacies will only prescribe certain COVID drugs, Paxlovid being one of them
- The key to getting away with a really big lie is making it so divorced from reality that the listener will assume their own perception is flawed, and then repeating it over and over again. This strategy has been used to great effect over the past three years, resulting in a massive shift from fact-based public health orthodoxy to irrational fantasy-based dogma
- Centralized top-down health care is far more attractive to Big Pharma investors than patient-centered care. The primary obstacle to the corporatization and monetization of public health has been truth, and this obstacle was finally overcome during the COVID pandemic
- The Big Lies told during the pandemic work because they veer so sharply from the truth. This break from factual reality is what makes it so difficult to question them, because if you do, you’re now questioning the entire hierarchy of public health
The manufactured COVID pandemic has been a proverbial golden egg-laying goose for Pfizer. Its annual revenue is expected to reach $101.3 billion in 2022,1 thanks to its COVID jab, which doesn’t prevent infection or spread, and Paxlovid, an ineffective and dangerous COVID antiviral that causes rebound. It would be comical if it weren’t so egregious.
And, Pfizer’s coffers are more or less guaranteed to continue being filled to the brim as the U.S. Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices (ACIP) has now added COVID-19 shots to the U.S. childhood, adolescent and adult vaccine schedules.2
With this action, the CDC has secured Pfizer’s (and Moderna’s) permanent liability shield so that no one can sue them for damages for injuries and deaths occurring as a result of the shots. It also opens the door for states to mandate the jab for school children, which guarantees a continuous revenue stream.
That revenue stream may even exceed previous profits, as Pfizer raised the price on its COVID jab by about 400%,3 from $304 per jab to somewhere between $110 and $130, on the same day ACIP voted to add the shot to the vaccine schedule. That price hike will take effect once the current U.S. purchase program expires.
Pfizer Hunts for the Next Blockbuster
As reported by Kaiser Health News (KHN),5 “a fortune amassed in the COVID pandemic is now paving the path to pharma nirvana: a weight loss pill likely worth hundreds of billions.” Pfizer is also hoping to develop blockbuster drugs for diabetes, migraines, ulcerative colitis, prostate cancer and sickle cell disease, and is gobbling up smaller drug companies with promising product portfolios.
A blockbuster drug may rake in billions, but that doesn’t mean it’s a blockbuster in the sense that it’s effective, as we’ve seen with Paxlovid and the mRNA COVID shot. Pfizer gets around this in large part by being a “remarkable marketing machine,” to quote Timothy Calkins, a professor of marketing at Northwestern University’s Kellogg School of Management.6
Not only is Pfizer spending big bucks on splashy advertising, they also work with contract research firms like ICON, which run medical research trials for drug companies and federal agencies alike, thereby giving the drug companies the inside track on drug approvals.7,8
Pfizer also gets plenty of free help from the federal government which, in the case of COVID, coerced millions with job loss threats into getting the shots, and implemented rules that ensure hospitals and pharmacies will only prescribe certain COVID drugs, Paxlovid being one of them.
The Art of Really Big Lies
In a November 4, 2022, article,9 clinical and public health physician Dr. David Bell discusses the art — and price — of lying, noting that the more divorced a lie is from reality, the more likely it is to succeed, thanks to the quirks of human nature and normal psychology:
“In a former role I had a boss who lied a lot. The lies were pure fantasy, but massive in scope and delivered with sincerity. They were very successful.
This success was based on the reluctance of most people to consider that someone in a position of authority in a humanitarian organization would completely ignore all semblance of reality. People assumed the claims must be true as fabricating information to that extent in those circumstances seemed to defy logic.
The principle of Really Big Lies is based on the lies being so divorced from reality that the listener will assume their own perception must be flawed, rather than doubt the claims of the person telling the lies. Only an insane or ridiculous person would make such outlandish claims, and a credible institution would not employ such a person.
Therefore, given that the institution is apparently credible, the statements must also be credible, and the listener’s prior perception of reality was therefore flawed. Lesser lies, by contrast, are likely to be perceived as sufficiently close to known reality to be demonstrably wrong. Inventing truth can be more effective than bending it.”
I believe this is precisely the strategy employed by Big Pharma, health agencies, government officials and the deep state propaganda arm over the past three years. Their claims have been so far from any semblance of reality, anyone aware of the facts has been left feeling more than a little crazy.
Unfortunately, while most humans have a moral and ethical compass, few end up following it when confronted by psychopaths in authority and the peer pressure to conform. As noted by Bell, good team players almost always end up supporting false narratives, and those who refuse to go along with what are clearly lies tend to be but a tiny minority.
Profit Through Deception
For decades, patient-centered health care has been the norm, and patients not only had the right, but the duty, to participate in the planning and implementation of their care. This was enshrined in the 1978 Declaration of Alma Ata10 — a declaration adopted by the World Health Organization “as the key to achieving an acceptable level of health throughout the world.”
However, as noted by Bell, centralized top-down health care is far more attractive to Big Pharma investors. The primary obstacle to the corporatization and monetization of public health was truth, and this obstacle was finally (and formidably) overcome during the COVID pandemic. Bell explains:11
“COVID-19 proved that even this impediment to progress can be expunged through consistent lying and the vilification of truth-tellers, backed by a well-managed behavioral psychology campaign.
This pandemic response provided a template not only for vastly-increased corporate income, but for job certainty and expansion of opportunity for the army of mostly-Western bureaucrats and health professionals filling the offices, meeting rooms and business-class seats of its implementing organizations. COVID-19 made corporate colonialism respectable again.
Superficially, COVID-19 appears a poor disease choice to facilitate a fundamental societal reset.
Death is heavily concentrated in old age ... Severe cases are generally confined to those with life expectancies already shortened by metabolic diseases ... Countries that failed to implement measures to restrict and impoverish their people ... had COVID-19 outcomes similar to those that opted for lockdowns and other trappings of medical fascism.
Average hospital admissions in the UK and USA declined during the pandemic, not what the public expects when a pathogen wreaks havoc. Lockdowns devastated economies ... COVID vaccines have also been unhelpful as high vaccination rates failed to noticeably impact infection and transmission ...
Thus, COVID-19 provided a hard bucket of facts to deal with, but this is just the situation in which Really Big Lies can work. These were needed both to fool the public, and to provide a structure within which health professionals could implement the policy.
Largely by playing on fear, divorcing data from context, and disseminating false information widely and incessantly, a whole new belief system has been constructed in public health to replace the evidence-based orthodoxy of former years.
Reality has been replaced with dogma so divorced from any basis in fact that it is easier to go with the propaganda than deal with the dissonance that would otherwise result.”
The New Fantasy-Based Dogmas
The new fantasy-based beliefs that health care workers, patients, researchers, academics and public health employees are now forced to embrace include the following, quoted from Bell’s article:12
- Disease burden should be measured in raw mortality, and not include metrics such as life-years lost. Hence an 85-year-old dying of a respiratory virus is equivalent to a 5-year-old dying of malaria in terms of burden and urgency;
- Medium and long-term harms due to poverty and reduced healthcare access should not be considered when assessing the value of an intervention. A modelled effect on the target pathogen is the only relevant metric;
- It is appropriate to misinform the public on age-related risk and relative disease burden and better to instill fear in order to achieve compliance with public-health directives;
- Growth of viral transmission in a community follows an exponential curve, rather than a steady deceleration (e.g. Gompertz curve) as the proportion of recovered (immune) people accumulate;
- Banning students from school for a year protects the elderly, while not locking in generational poverty;
- Cloth and surgical masks stop aerosolized virus transmission, and all meta-analyses of randomized control trials (that show minimal or no effect) should be ignored;
- Post-infection immunity to respiratory viruses is expected to be poor and short-lived, whilst vaccines to a single viral protein will somehow produce much stronger immunity;
- Immunity to viruses is best measured by antibody concentrations rather than T-cell response or clinical outcomes;
- Informed consent for vaccination should not include information on demonstrated risks, as this could promote ‘vaccine hesitancy’;
- It is appropriate to give a new gene-based pharmaceutical class in pregnancy that crosses the placenta without any pregnancy trial data, toxicology studies, or long-term outcomes data (in anyone);
- Irrespective of the Convention on the Rights of the Child ‘In all actions concerning children … the best interests of the child shall be a primary consideration,’ it is appropriate to inject children with drugs lacking long-term safety data in order to protect the elderly;
- Pandemics are becoming more frequent and more deadly, despite the historical record, and the progress of modern medicine, indicating quite the opposite.
Refusing the False Narratives Has Real Consequences
As Bell correctly points out, these new public health positions are not just slightly incorrect. They’re all “either unethical or clear nonsense, contradicted by prior public health orthodoxy.” Indeed, most are classical Orwellian doublespeak and 180 degrees from the truth.
But it’s the sharp break from factual reality that makes it impossible to question them because, if you do, you’re now questioning “the entire current hierarchy of public health,” Bell says.
To quote Dr. Anthony Fauci, you’re not attacking him when you question his irrational flip-flopping, you’re questioning science itself. If you question any of these fantasy-based beliefs, you’re now a science-denier, and you’re putting your employment and reputation at risk. Unfortunately, those risks are not imaginary.
The way out of this is simply to refuse to lie, or cover for the lies of others ... [The] truth will catch up, one day, with those who don’t ... It is far better to leave early and live with dignity. ~ Dr. David Bell
The punishment for refusing these false narratives is very real and very severe. Many doctors and scientists whose reputations and contributions to public health have been beyond reproach for decades have been stripped of their medical licenses and lost their jobs for speaking out against these COVID fallacies.
So, where do we go from here? How do we end the madness and return to reality-based public health?
“Whilst growing their industry’s finances, public health professionals are degrading themselves and betraying society,” Bell writes.13 “The betrayal, based on incessant lying, is something for which they will inevitably face consequences ...
Eventually, even the most dedicated followers will begin to question the sense of putting on a mask at a restaurant door only to remove it 10 steps later, or vaccinating vast populations against a disease to which they are already immune whilst they die of other readily preventable diseases.
The way out of this is simply to refuse to lie, or cover for the lies of others ... [The] truth will catch up, one day, with those who don’t ... It is far better to leave early and live with dignity.”
Evil Genius: Creating the Market
If you’re paying attention, you’ve undoubtedly noticed that many drug companies, Pfizer in particular, are in the business of creating their own markets. Pfizer released a COVID jab that neither protects against infection nor prevents spread, thereby necessitating multiple boosters. Its antiviral COVID drug Paxlovid causes rebound, necessitating multiple doses.
Now we find that the COVID jabs are also associated with increased rates of respiratory syncytial virus (RSV) infection in children, and like clockwork, Pfizer and Moderna start working on RSV jabs. The CDC also aids by recommending kids get additional COVID shots. Is this a racket or what!?
The Informed Consent Action Network (ICAN) is now demanding answers from the CDC about the off-season spike in RSV rates,14 which mysteriously arose in the wake of childhood injections against COVID.
Moderna’s pediatric COVID jab trial showed those who got the jab had higher rates of RSV than the placebo group. RSV was also one of the primary serious side effects in Pfizer’s pediatric trial. Now, all of a sudden, we’re seeing out-of-season RSV spikes in children. Coincidence? Make them prove it. In a legal update, ICAN reports:
“The issue is so serious that even the FDA’s vaccine committee, VRBPAC, which normally cheerleads even the most dangerous vaccine, noted the correlation and ‘stressed the importance of continued post-authorization safety surveillance, in particular for … certain respiratory infections (RSV and pneumonia) in the youngest age group ...’15
Despite the noted importance of surveilling RSV post-authorization, no one at CDC or FDA seems to be drawing a connection between the increase in RSV and the COVID-19 vaccines being administered to children.
Incredibly, the CDC just issued an ‘Official Health Advisory’16 about the increase RSV and respiratory virus cases and, in it, the CDC recommends all individuals 6 months and up receive an influenza vaccine and a COVID-19 vaccine!
Not surprisingly, the press has missed the mark, too. While there are numerous articles detailing the troubling increase in sick children, none reference COVID-19 vaccination despite the data from the manufacturers’ trials.
To get to the bottom of this, on October 26, 2022, ICAN’s attorneys sent a letter17 to the CDC observing the clinical trial data showing a correlation between increased RSV cases and receipt of a COVID-19 vaccine. ICAN’s letter demanded to know the percentage of children who tested positive for RSV and who had received a COVID-19 vaccine prior to their RSV diagnosis.”
Study Calls for Reevaluation of Jab Campaigns
In related news, we also have a November 2022 study18 in Nature Communications, which questions the rationale of current booster campaigns. According to the authors:
“An important aspect of vaccine effectiveness is its impact on pathogen transmissibility, harboring major implications for public health policies. As viral load is a prominent factor affecting infectivity, its laboratory surrogate, qRT-PCR cycle threshold (Ct), can be used to investigate the infectivity-related component of vaccine effectiveness ...
By analyzing results of more than 460,000 individuals, we show that while recent vaccination reduces Omicron viral load, its effect wanes rapidly. In contrast, a significantly slower waning rate is demonstrated for recovered COVID-19 individuals.
Thus, while the vaccine is effective in decreasing morbidity and mortality, its relatively small effect on transmissibility of Omicron (as measured here by Ct) and its rapid waning call for reassessment of future booster campaigns.”
Considering the theoretical protection of these shots last for just 70 days (according to this study), are the risks associated with the shots really worth it? So far, several risk-benefit analyses have all come to the conclusion that the risks far outweigh any potential benefit.
Unfortunately, it seems we have to rely on scientists outside the U.S. to do this kind of bench science, as all we seem get from American research institutions are analyses of how to get “anti-vaxxers” to buy the false narrative and roll up their sleeves.
About
© 2025 Created by carol ann parisi.
Powered by
![]()